Systemic Sclerosis (Scleroderma)
Definition:
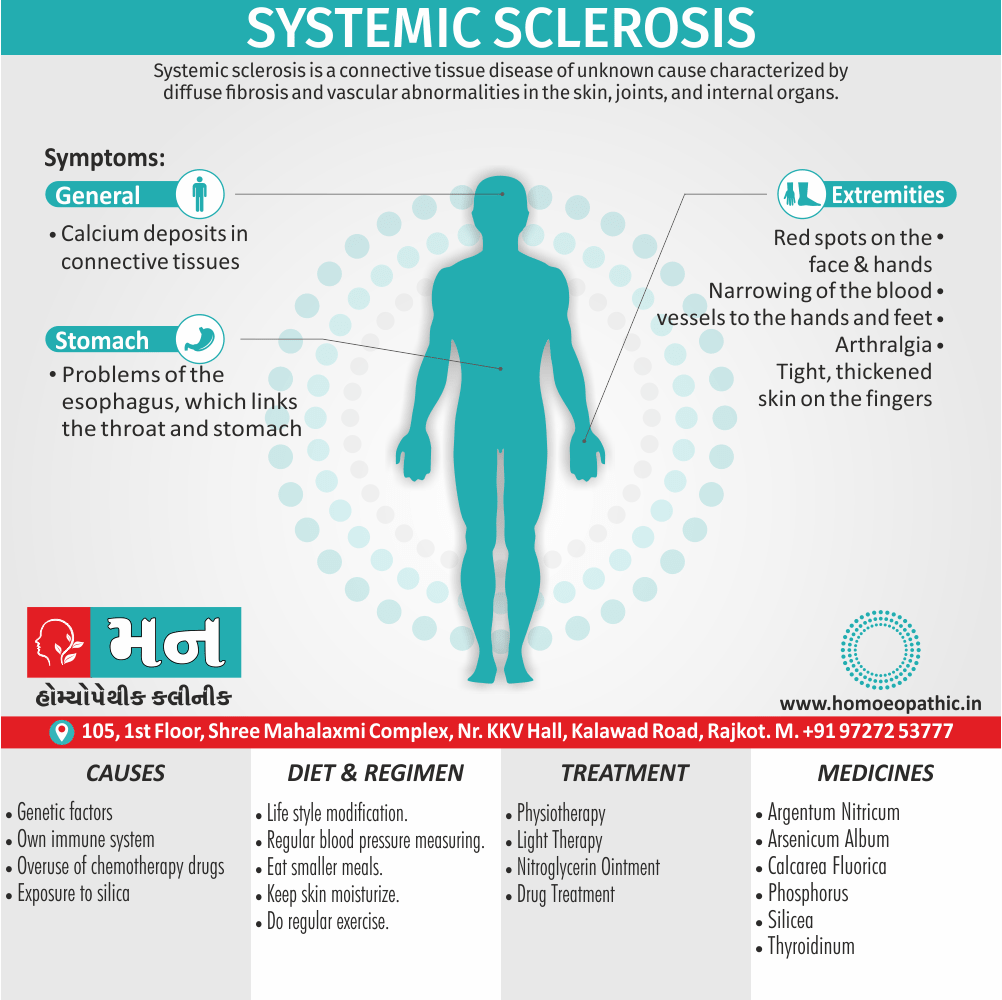
Systemic sclerosis is a connective tissue disease of unknown cause characterized by diffuse fibrosis and vascular abnormalities in the skin, joints, and internal organs. [3]
Overview of Systemic Sclerosis
- Basically, Scleroderma refers to a range of disorders in which the skin and connective tissues tighten and harden.
- That is a long-term, progressive disease also gradually gets worse.
- It is consider a rheumatic disease and a connective tissue disorder.
- This is also thought to be an autoimmune condition, in which the body’s own immune system attacks the body’s tissues.
- This results in an overproduction of collagen, the protein that forms the basis of connective tissue.
- The result is a thickening, or fibrosis, also scarring of tissue.
- Furthermore, Scleroderma is not contagious.
- And may run in families, but it often occurs in patients without any family history of the disease.
- It is thought to affect between 75,000 and 100,000 people in the United States, mostly women aged from 30 to 50 years. [2]
- Besides this, There is characterise by sclerodactyly in combination with Raynaud’s and digital ischaemia.
- The peak age of onset is in the fourth and fifth decades, and overall prevalence is 10–20 per 100 000, with a 4 : 1 female preponderance.
- All in all, That is subdivide into diffuse cutaneous systemic sclerosis & limited cutaneous systemic sclerosis. [1]
It is sometimes known as CREST syndrome, because the symptoms form the acronym, CREST i.e.:
- C: Calcinosis, or calcium deposits in tissues and under the skin
- R: Raynaud’s disease
- E: Esophageal problems, including GERD
- S: Sclerodactyly, or thick skin on the fingers
- T: Telangiectasias, or enlarged blood vessels, manifesting as red spots [2]
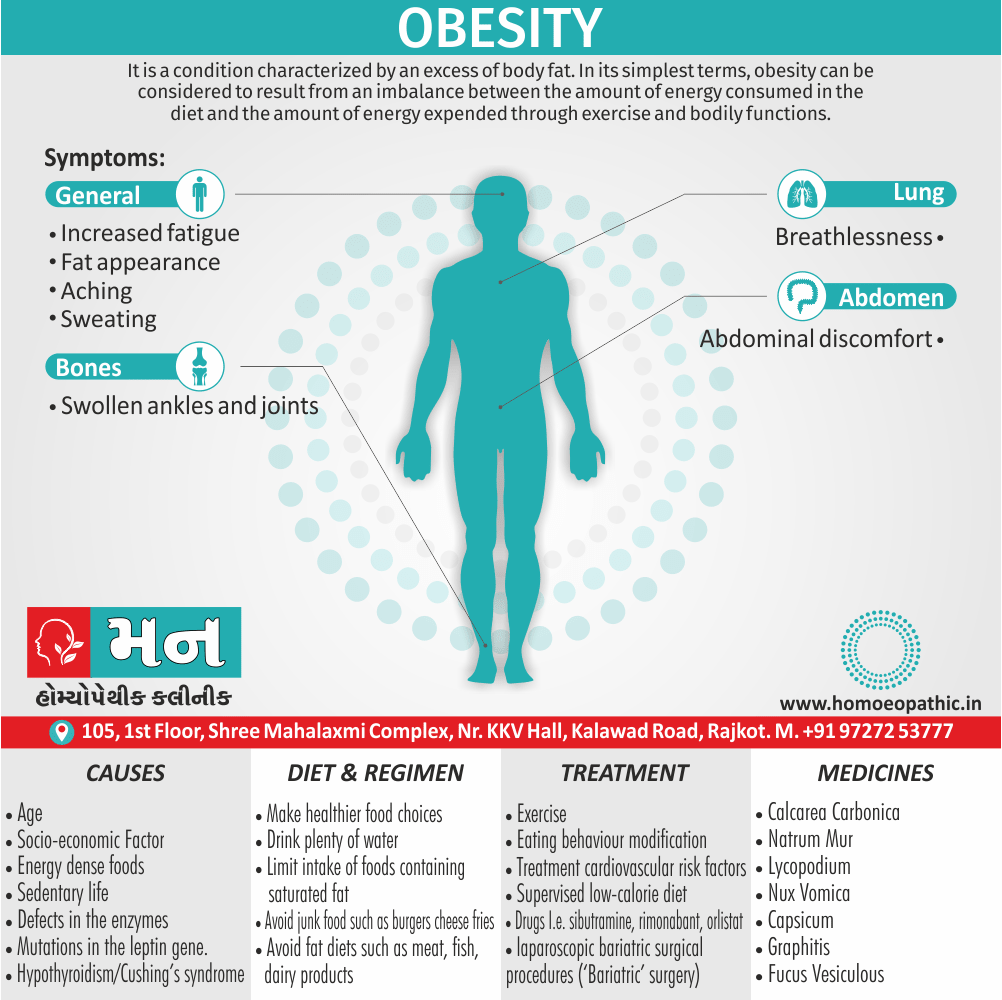
Sign & Symptoms of Systemic Sclerosis
Scleroderma
Skin:
- Initially, there is non pitting oedema of fingers and flexor tendon sheaths.
- Subsequently, the skin becomes shiny and taut, and distal skin creases disappear.
- This is accompany by erythema and tortuous dilatation of capillary loops in the nailfold bed, readily visible with an ophthalmoscope or dissecting microscope (and oil placed on the skin).
- The face and neck are usually involve next, with thinning of the lips and radial furrowing.
- Moreover, In some patients, skin thickening stops at this stage.
- Skin involvement restricted to sites distal to the elbow or knee (apart from the face) is classifying as ‘limited disease’ or CREST syndrome.
- Involvement proximal to the knee and elbow and on the trunk is classified as ‘diffuse disease’.
Raynaud’s phenomenon:
- This is a universal feature also can precede other features by many years.
- Involvement of small blood vessels in the extremities may cause critical tissue ischaemia, leading to skin ulceration over pressure areas, localised areas of infarction and pulp atrophy at the fingertips.
Musculoskeletal features:
- Arthralgia, morning stiffness also flexor tenosynovitis are common.
- Restricted hand function is due to skin rather than joint disease also erosive arthropathy is uncommon.
- Muscle weakness and wasting can occur due to myositis.
Gastrointestinal Involvement:
- Smooth muscle atrophy and fibrosis in the lower two thirds of the oesophagus lead to reflux with erosive oesophagitis.
- Furthermore, Dysphagia and odynophagia may also occur.
- Involvement of the stomach causes early satiety and occasionally outlet obstruction.
- Recurrent occult upper gastrointestinal bleeding may indicate a ‘watermelon’ stomach (antral vascular ectasia), which occurs in up to 20% of patients.
- Besides this, Small intestine involvement may lead to malabsorption due to bacterial overgrowth and intermittent bloating, pain or constipation.
- Lastly, Dilatation of large or small bowel due to autonomic neuropathy may cause pseudo obstruction with nausea, vomiting, abdominal discomfort and distension, often worse after food.
Pulmonary Involvement:
- This is a major cause of morbidity also mortality.
- Pulmonary hypertension complicates long standing disease and is six times more prevalent in LCSS than in DCSS.
- It presents with rapidly progressive dyspnoea (more rapid than interstitial lung disease), right heart failure also angina, often in association with severe digital ischaemia.
- Fibrosing alveolitis mainly affects patients with DCSS who have topoisomerase 1 antibodies.
Renal involvement:
- In brief, One of the main causes of death is hypertensive renal crisis, characterised by rapidly developing malignant hypertension and renal failure. [1]
Causes of Systemic Sclerosis
- It is not known what causes scleroderma, but it is thought to an autoimmune condition that causes the body to produce too much connective tissue.
- This leads to a thickening, or fibrosis, and scarring of tissue.
- Connective tissue forms the fibers that make up the framework that supports the body.
- They are found under the skin and around the internal organs and blood vessels, and they help support muscles and bones.
- Genetic factors are thought to play a role, and possibly environmental factors, but this has not confirmed.
- People with scleroderma often come from families in which another autoimmune disease exists.
- It is not contagious. [2]
Risk Factors:
Risk factors that can increase your chances of developing the condition include i.e.:
- Being Native American / African American
- Being female
- Using certain chemotherapy drugs such as Bleomycin
- Exposed to silica dust also organic solvents
There’s no known way to prevent SS other than to reduce risk factors you can control. [4]
Diagnosis of Systemic Sclerosis
Scleroderma is primarily a clinical diagnosis but various laboratory abnormalities are characteristic.
The ESR is usually elevate also raised levels of IgG are common, but CRP values tend to be normal unless there is severe organ involvement or coexisting infection.
ANA is positive in about 70%, and approximately 30% of patients with DCSS have antibodies to topoisomerase 1 (Scl70).
About 60% of patients with CREST syndrome have anticentromere antibodies. [1]
The following tests may be necessary:
- Looking at the skin under a microscope to check for changes either in the tiny blood vessels, or capillaries, around the fingernails
- Skin biopsy
- Blood tests to assess the levels of certain antibodies [2]
Treatment of Systemic Sclerosis
No treatments are available that either halt or reverse the fibrotic changes that underlie the disease.
The focus of management, therefore, is to ameliorate the effects of the disease on target organs.
Treatment for generalized symptoms may involve:
- Corticosteroids
- Immunosuppressants, such as methotrexate or Cytoxan
- Nonsteroidal anti-inflammatory drugs (in other words, NSAID)
Depending on your symptoms, treatment can also include:
- Blood pressure medication
- Medication to aid breathing
- Physical therapy
- Light therapy, such as ultraviolet A1 phototherapy
- Nitroglycerin ointment to treat localized areas of tightening of the skin [4]
Raynaud’s syndrome & Digital ulcers i.e.:
- Raynaud’s should treat by avoidance of cold exposure and use of mittens (heated mittens are available), supplemented if necessary with calcium antagonists.
- Intermittent infusions of prostacyclin may benefit severe digital ischaemia.
- The endothelin 1 antagonist bosentan can be of value in promoting healing of digital ulcers.
- If these become infected, antibiotics may required, but as these penetrate tissues poorly in scleroderma, they need to be given at higher doses for a longer duration than usual.
Oesophageal Reflux i.e.:
- It should treated with proton pump inhibitors and antireflux agents.
- Antibiotics may required for bacterial overgrowth syndromes, and metoclopramide or domperidone may help patients with symptoms of pseudo obstruction.
Hypertension i.e.:
- It should be treated aggressively with ACE inhibitors, even if renal impairment is present.
Joint involvement i.e.:
- This may be treated with analgesics and/or NSAID.
- If synovitis is present, immunosuppressants such as methotrexate can also be of value.
Pulmonary Hypertension i.e.:
- This may be treated with bosentan.
- In selected patients, heart–lung transplantation may be considered.
- Corticosteroids and cytotoxic drugs are indicated in patients who have coexisting myositis or fibrosing alveolitis. [1]
Homeopathic Treatment of Systemic Sclerosis
Argentum Nitricum:
- Pale face.
- Tight drawing of skin over bones.
- Skin becomes brown, tense, dry also hard.
- Drawing in skin as from a either spider web or dried albuminous substance.
- Irregular blotches.
- Worse by warmth in any form, at night, left side.
- Better especially in fresh air & cold.
Arsenicum Album:
- Face: Swollen, pale, sunken, cold.
- Throat: Swollen, oedematous, constricted, unable to swallow.
- Extremities: Swelling of feet.
- Skin: Swellings, oedema, gangrenous inflammations.
- Worse: Cold, wet weather.
- Better: Heat.
Calcarea Fluorica:
- Face: Hard swelling on cheek also jaw bone with pain.
- Extremities: Gouty enlargements of finger joints.
- Skin: Indurations of stony hardness.
- Worse: During rest, changes of weather.
- Better: Heat.
Phosphorus:
- Skin: Tightness on forehead.
- Face: Pale, sickly complexion, blue rings especially under eyes. Swelling also necrosis of lower jaw.
- Extremities: Ascending sensory also motor paralysis from ends of fingers also toes. In detail, Numbness in hands.
- Worse: Touch, physical or mental exertion, change of weather, from getting wet in hot weather.
- Better: specifically Cold, open air, washing with cold water.
Silicea:
- Skin: Delicate, pale, waxy. In detail, Dry fingertips.
- Worse: In morning, from washing, damp cold weather.
- Better: Warmth, summer, either in wet or humid weather.
Thyroidinum:
- Skin: Dry. Additionally, Swelling of glands of stony hardness.
- Worse: Night. [5]
Frequently Asked Questions
What is Systemic Sclerosis?
Systemic sclerosis is a connective tissue disease of unknown cause characterized by diffuse fibrosis and vascular abnormalities in the skin, joints, and internal organs.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Systemic Sclerosis?
- Argentum Nitricum
- Arsenicum Album
- Calcarea Fluorica
- Phosphorus
- Silicea
- Thyroidinum
What causes Systemic Sclerosis?
- Autoimmune
- Genetic factors
- Using certain chemotherapy drugs
- Exposed to silica dust
- Come from families
What are the symptoms of Systemic Sclerosis?
- Non pitting oedema of fingers and flexor tendon sheaths
- Shiny and taut
- Erythema and tortuous dilatation of capillary loops
- Raynaud’s phenomenon
- Arthralgia, morning stiffness
- Restricted hand function
- Davidson’s Principles and Practice of Medicine (22nd edition) Ch. 25
- https://www.medicalnewstoday.com/articles/176357.php
- https://www.msdmanuals.com/professional/musculoskeletal-and-connective-tissue-disorders/autoimmune-rheumatic-disorders/systemic-sclerosis
- https://www.healthline.com/health/scleroderma#symptoms
- Zomeo Ultimate LAN 3.0
Definition:
Systemic sclerosis is a connective tissue disease of unknown cause characterized by diffuse fibrosis and vascular abnormalities in the skin, joints, and internal organs. [3]
Overview
Epidemiology
Causes
Risk Factors
Pathogenesis
Pathophysiology
Types
Clinical Features
Sign & Symptoms
Clinical Examination
Diagnosis
Differential Diagnosis
Complications
Investigations
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Terminology
References
FAQ
Also Search As
Overview
Overview of Systemic Sclerosis
- Basically, Scleroderma refers to a range of disorders in which the skin and connective tissues tighten and harden.
- That is a long-term, progressive disease also gradually gets worse.
- It is consider a rheumatic disease and a connective tissue disorder.
- This is also thought to be an autoimmune condition, in which the body’s own immune system attacks the body’s tissues.
- This results in an overproduction of collagen, the protein that forms the basis of connective tissue.
- The result is a thickening, or fibrosis, also scarring of tissue.
- Furthermore, Scleroderma is not contagious.
- And may run in families, but it often occurs in patients without any family history of the disease.
- It is thought to affect between 75,000 and 100,000 people in the United States, mostly women aged from 30 to 50 years. [2]
- Besides this, There is characterise by sclerodactyly in combination with Raynaud’s and digital ischaemia.
- The peak age of onset is in the fourth and fifth decades, and overall prevalence is 10–20 per 100 000, with a 4 : 1 female preponderance.
- All in all, That is subdivide into diffuse cutaneous systemic sclerosis & limited cutaneous systemic sclerosis. [1]
It is sometimes known as CREST syndrome, because the symptoms form the acronym, CREST i.e.:
- C: Calcinosis, or calcium deposits in tissues and under the skin
- R: Raynaud’s disease
- E:Esophageal problems, including GERD
- S: Sclerodactyly, or thick skin on the fingers
- T: Telangiectasias, or enlarged blood vessels, manifesting as red spots [2]
Epidemiology
Indian epidemiology then other
Causes
Causes of Systemic Sclerosis
- It is not known what causes scleroderma, but it is thought to an autoimmune condition that causes the body to produce too much connective tissue.
- This leads to a thickening, or fibrosis, and scarring of tissue.
- Connective tissue forms the fibers that make up the framework that supports the body.
- They are found under the skin and around the internal organs and blood vessels, and they help support muscles and bones.
- Genetic factors are thought to play a role, and possibly environmental factors, but this has not confirmed.
- People with scleroderma often come from families in which another autoimmune disease exists.
- It is not contagious. [2]
Risk Factors:
Risk factors that can increase your chances of developing the condition include i.e.:
- Being Native American / African American
- Being female
- Using certain chemotherapy drugs such as Bleomycin
- Exposed to silica dust also organic solvents
There’s no known way to prevent SS other than to reduce risk factors you can control. [4]
Risk Factors
Risk factors are things that make you more likely to develop a disease in the first place.
Pathogenesis
Pathogenesis refers to the development of a disease. It’s the story of how a disease gets started and progresses.
This is the entire journey of a disease, encompassing the cause but going beyond it.
Pathophysiology
Pathophysiology, on the other hand, focuses on the functional changes that occur in the body due to the disease. It explains how the disease disrupts normal physiological processes and how this disruption leads to the signs and symptoms we see.
Imagine a car accident. Pathogenesis would be like understanding how the accident happened – what caused it, the sequence of events (e.g., one car ran a red light, then hit another car). Pathophysiology would be like understanding the damage caused by the accident – the bent fenders, deployed airbags, and any injuries to the passengers.
In simpler terms, pathogenesis is about the "why" of a disease, while pathophysiology is about the "how" of the disease’s effects.
Types
AAA
Clinical Features
Tab Content
Sign & Symptoms
Sign & Symptoms of Systemic Sclerosis
Scleroderma
Skin:
- Initially, there is non pitting oedema of fingers and flexor tendon sheaths.
- Subsequently, the skin becomes shiny and taut, and distal skin creases disappear.
- This is accompany by erythema and tortuous dilatation of capillary loops in the nailfold bed, readily visible with an ophthalmoscope or dissecting microscope (and oil placed on the skin).
- The face and neck are usually involve next, with thinning of the lips and radial furrowing.
- Moreover, In some patients, skin thickening stops at this stage.
- Skin involvement restricted to sites distal to the elbow or knee (apart from the face) is classifying as ‘limited disease’ or CREST syndrome.
- Involvement proximal to the knee and elbow and on the trunk is classified as ‘diffuse disease’.
Raynaud’s phenomenon:
- This is a universal feature also can precede other features by many years.
- Involvement of small blood vessels in the extremities may cause critical tissue ischaemia, leading to skin ulceration over pressure areas, localised areas of infarction and pulp atrophy at the fingertips.
Musculoskeletal features:
- Arthralgia, morning stiffness also flexor tenosynovitis are common.
- Restricted hand function is due to skin rather than joint disease also erosive arthropathy is uncommon.
- Muscle weakness and wasting can occur due to myositis.
Gastrointestinal Involvement:
- Smooth muscle atrophy and fibrosis in the lower two thirds of the oesophagus lead to reflux with erosive oesophagitis.
- Furthermore, Dysphagia and odynophagia may also occur.
- Involvement of the stomach causes early satiety and occasionally outlet obstruction.
- Recurrent occult upper gastrointestinal bleeding may indicate a ‘watermelon’ stomach (antral vascular ectasia), which occurs in up to 20% of patients.
- Besides this, Small intestine involvement may lead to malabsorption due to bacterial overgrowth and intermittent bloating, pain or constipation.
- Lastly, Dilatation of large or small bowel due to autonomic neuropathy may cause pseudo obstruction with nausea, vomiting, abdominal discomfort and distension, often worse after food.
Pulmonary Involvement:
- This is a major cause of morbidity also mortality.
- Pulmonary hypertension complicates long standing disease and is six times more prevalent in LCSS than in DCSS.
- It presents with rapidly progressive dyspnoea (more rapid than interstitial lung disease), right heart failure also angina, often in association with severe digital ischaemia.
- Fibrosing alveolitis mainly affects patients with DCSS who have topoisomerase 1 antibodies.
Renal involvement:
- In brief, One of the main causes of death is hypertensive renal crisis, characterised by rapidly developing malignant hypertension and renal failure. [1]
Clinical Examination
Tab Content
Diagnosis
Diagnosis of Systemic Sclerosis
Scleroderma is primarily a clinical diagnosis but various laboratory abnormalities are characteristic.
The ESR is usually elevate also raised levels of IgG are common, but CRP values tend to be normal unless there is severe organ involvement or coexisting infection.
ANA is positive in about 70%, and approximately 30% of patients with DCSS have antibodies to topoisomerase 1 (Scl70).
About 60% of patients with CREST syndrome have anticentromere antibodies. [1]
The following tests may be necessary:
- Looking at the skin under a microscope to check for changes either in the tiny blood vessels, or capillaries, around the fingernails
- Skin biopsy
- Blood tests to assess the levels of certain antibodies [2]
Differential Diagnosis
Complications
Complications are what happen after you have a disease. They are the negative consequences of the disease process.
Investigations
Tab Content
Treatment
Treatment of Systemic Sclerosis
No treatments are available that either halt or reverse the fibrotic changes that underlie the disease.
The focus of management, therefore, is to ameliorate the effects of the disease on target organs.
Treatment for generalized symptoms may involve:
- Corticosteroids
- Immunosuppressants, such as methotrexate or Cytoxan
- Nonsteroidal anti-inflammatory drugs (in other words, NSAID)
Depending on your symptoms, treatment can also include:
- Blood pressure medication
- Medication to aid breathing
- Physical therapy
- Light therapy, such as ultraviolet A1 phototherapy
- Nitroglycerin ointment to treat localized areas of tightening of the skin [4]
Raynaud’s syndrome & Digital ulcers i.e.:
- Raynaud’s should treat by avoidance of cold exposure and use of mittens (heated mittens are available), supplemented if necessary with calcium antagonists.
- Intermittent infusions of prostacyclin may benefit severe digital ischaemia.
- The endothelin 1 antagonist bosentan can be of value in promoting healing of digital ulcers.
- If these become infected, antibiotics may required, but as these penetrate tissues poorly in scleroderma, they need to be given at higher doses for a longer duration than usual.
Oesophageal Reflux i.e.:
- It should treated with proton pump inhibitors and antireflux agents.
- Antibiotics may required for bacterial overgrowth syndromes, and metoclopramide or domperidone may help patients with symptoms of pseudo obstruction.
Hypertension i.e.:
- It should be treated aggressively with ACE inhibitors, even if renal impairment is present.
Joint involvement i.e.:
- This may be treated with analgesics and/or NSAID.
- If synovitis is present, immunosuppressants such as methotrexate can also be of value.
Pulmonary Hypertension i.e.:
- This may be treated with bosentan.
- In selected patients, heart–lung transplantation may be considered.
- Corticosteroids and cytotoxic drugs are indicated in patients who have coexisting myositis or fibrosing alveolitis. [1]
Prevention
Tab Content
Homeopathic Treatment
Homeopathic Treatment of Systemic Sclerosis
Argentum Nitricum:
- Pale face.
- Tight drawing of skin over bones.
- Skin becomes brown, tense, dry also hard.
- Drawing in skin as from a either spider web or dried albuminous substance.
- Irregular blotches.
- Worse by warmth in any form, at night, left side.
- Better especially in fresh air & cold.
Arsenicum Album:
- Face: Swollen, pale, sunken, cold.
- Throat: Swollen, oedematous, constricted, unable to swallow.
- Extremities: Swelling of feet.
- Skin: Swellings, oedema, gangrenous inflammations.
- Worse: Cold, wet weather.
- Better: Heat.
Calcarea Fluorica:
- Face: Hard swelling on cheek also jaw bone with pain.
- Extremities: Gouty enlargements of finger joints.
- Skin: Indurations of stony hardness.
- Worse: During rest, changes of weather.
- Better: Heat.
Phosphorus:
- Skin: Tightness on forehead.
- Face: Pale, sickly complexion, blue rings especially under eyes. Swelling also necrosis of lower jaw.
- Extremities: Ascending sensory also motor paralysis from ends of fingers also toes. In detail, Numbness in hands.
- Worse: Touch, physical or mental exertion, change of weather, from getting wet in hot weather.
- Better: specifically Cold, open air, washing with cold water.
Silicea:
- Skin: Delicate, pale, waxy. In detail, Dry fingertips.
- Worse: In morning, from washing, damp cold weather.
- Better: Warmth, summer, either in wet or humid weather.
Thyroidinum:
- Skin: Dry. Additionally, Swelling of glands of stony hardness.
- Worse: Night. [5]
Diet & Regimen
Do’s and Dont’s
Tab Content
Terminology
Tab Content
References
- Davidson’s Principles and Practice of Medicine (22nd edition) Ch. 25
- https://www.medicalnewstoday.com/articles/176357.php
- https://www.msdmanuals.com/professional/musculoskeletal-and-connective-tissue-disorders/autoimmune-rheumatic-disorders/systemic-sclerosis
- https://www.healthline.com/health/scleroderma#symptoms
- Zomeo Ultimate LAN 3.0
FAQ
Frequently Asked Questions
What is Systemic Sclerosis?
Systemic sclerosis is a connective tissue disease of unknown cause characterized by diffuse fibrosis and vascular abnormalities in the skin, joints, and internal organs.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Systemic Sclerosis?
- Argentum Nitricum
- Arsenicum Album
- Calcarea Fluorica
- Phosphorus
- Silicea
- Thyroidinum
What causes Systemic Sclerosis?
- Autoimmune
- Genetic factors
- Using certain chemotherapy drugs
- Exposed to silica dust
- Come from families
What are the symptoms of Systemic Sclerosis?
- Non pitting oedema of fingers and flexor tendon sheaths
- Shiny and taut
- Erythema and tortuous dilatation of capillary loops
- Raynaud’s phenomenon
- Arthralgia, morning stiffness
- Restricted hand function
Also Search As
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
How can I find reputable homeopathy clinics or homeopathic doctors in my area?
You can found Homeopathic Clinic For XXXX by searching for
Specific city Examples are
You can also search for near you Examples are