Deliberate Self-harm
Definition:
Deliberate self-harm is not usually fail suicide. Only about a quarter of those who have deliberately harmed themselves say they wished to die; most say the act was impulsive rather than premeditated.
The rest find it difficult to explain the reasons or say that:
They were seeking unconsciousness as a temporary escape or relief from their problems;
They were trying to influence another person to change their behaviour (e.g. to make a partner feel guilty about threatening to end the relationship);
Patient are uncertain whether or not they intended to die they were ‘leaving it to fate’;
Deliberate self-harm is common and rates have risen progressively over the last 30 years.
It now accounts for about 10 percent of acute medical admissions in the UK.
A further smaller number are see by general practitioners but not sent to hospital because the medical risks are low, or attend emergency departments but are not admitted.
Epidemiological studies have shown the kind of people who are more likely to harm themselves and the methods that are common.
Deliberate self-harm is more common among:
- younger adults: the rates decline sharply during adult life (they are also very low in children under the age of 12 years);
- young women, particularly those aged 15–20 years;
- people of low socioeconomic status;
- divorced individuals, teenage wives, and younger single adults.
Drug Overdose:
- In the UK, about 90 percent of the cases of deliberate self-harm treated by general hospitals involve drug overdose.
- The drugs taken most commonly in overdose are anxiolytics, non-opiate analgesics, such as salicylates and paracetamol, and antidepressants.
- Paracetamol is particularly dangerous because it damages the liver and may lead to delayed death, sometimes in patients who had not taken the drugs with the intention of dying.
- Antidepressants are take in about a fifth of cases.
- Of these drugs, tricyclics are particularly hazardous in overdosage since they may cause cardiac arrhythmias or convulsions.
- Despite these and other dangers, most deliberate drug overdoses do not present a serious threat to life.
The use of alcohol:
- About half of the men and a quarter of the women who harm themselves have taken alcohol within 6 hours before the act.
- This often precipitates the act by reducing self-restraint.
- Lastly, Its effects interact with those of the drugs.
Self Injury:
- In the UK, between 5 and 15 percent of all cases of deliberate self-harm treat in general hospitals are self-inflicted injuries.
- Moreover, Most of these injuries are lacerations, usually of the forearm or wrist.
- Most patients who cut themselves are young, have low self-esteem, impulsive or aggressive behaviour, unstable moods, difficulty in interpersonal relationships, also often problems of either alcohol or drug abuse.
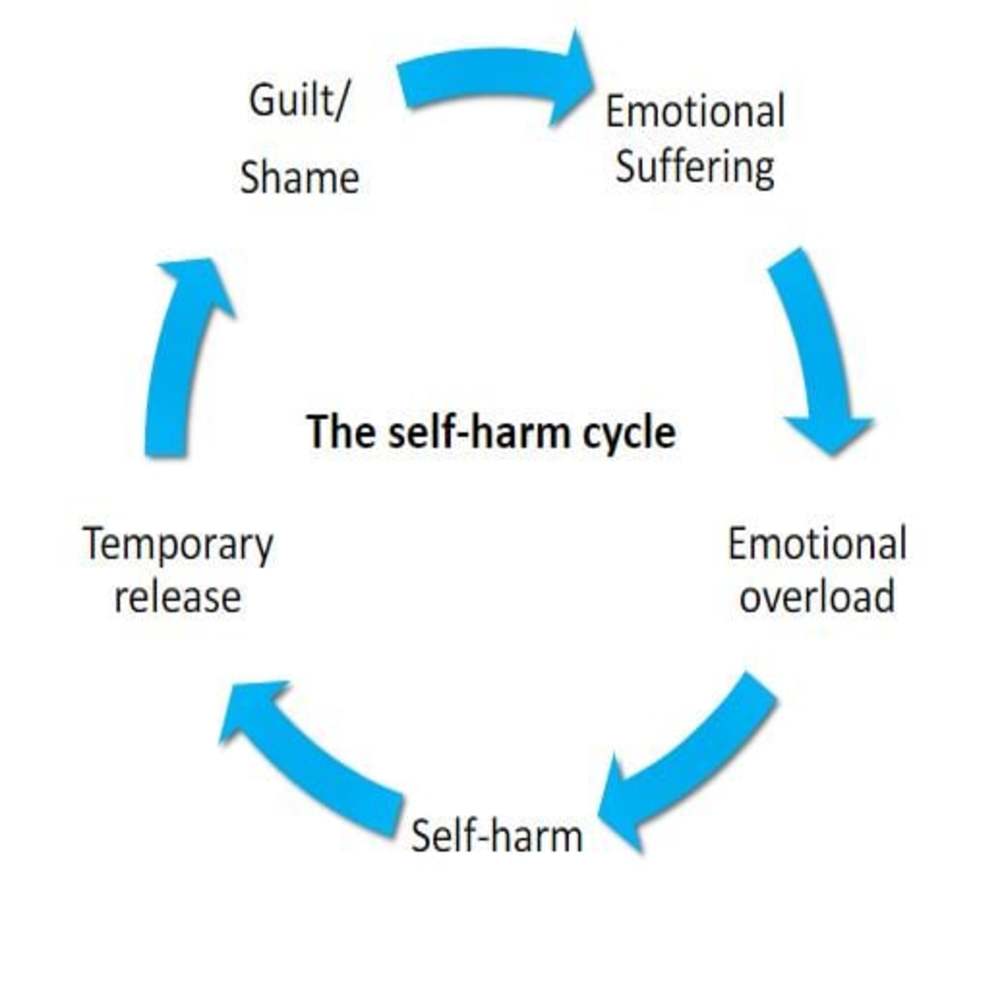
- Basically, the self-laceration follows a period of increasing tension and irritability which is relieve by the self-injury.
- Besides this, The cuts are usually multiple and superficial, often made with a razor blade or a piece of glass.
- All in all, These highly dangerous acts occur mainly among people who intended to die but have survived.
Less frequent and medically more serious forms of self injury i.e.:
- Deeper lacerations,
- Jumping from heights
- Jumping in front of a either moving train or motor vehicle
- Shooting
- Drowning
- Burning
Deliberate self-harm is usually the result of multiple social and personal factors, including national and local attitudes.
Overall, rates appear to be affected by awareness of the occurrence and methods of self-harm in a population (for example, television and press reports and local knowledge of suicide and attempted suicide in the neighbourhood).
Some causes of deliberate self-harm:
- Psychiatric disorder
- Personality disorder
- Alcohol dependence
- Predisposing social factors
- Early parental loss
- Parental neglect or abuse
- Long-term social problems: e.g. family, employment, financial
- Poor physical health
- Precipitating social factors
- Stressful life problems
Social and family factors:
Predisposing factors such as:
- Basically, Evidence of childhood emotional deprivation is common.
- Many patients who harm themselves have long-term marital problems, extramarital relationships, or other relationship problems, also may have financial and other social difficulties.
- Lastly, Rates of unemployment are greater than in the general population.
Precipitating factors such as:
- Stressful life events are frequent before the act of self-harm, especially quarrels with or threats of rejection by spouses or sexual partners.
Association with psychiatric disorder:
- Although many patients who harm themselves are anxious or depressed, relatively few have a psychiatric disorder other than an acute stress reaction, adjustment disorder, or personality disorder.
- The latter is found in about a third to a half of self-harm patients, and dependence on alcohol is also frequent. (In contrast, psychiatric disorder is common among patients who die by suicide.)
Difference between suicide & deliberate self-harm:
| Suicide | Deliberate self-harm | |
|
Age |
Older | Younger |
|
Sex |
More often male | More often female |
|
Psychiatric disorder |
Common, severe | Less common, less severe |
|
Physical illness |
Common | Uncommon |
|
Planning |
Careful | Impulsive |
|
Method |
Lethal | Less dangerous |
Since deliberate self-harm results from long-term adverse social factors and is associate with personality disorder, it is not surprising that a significant proportion of subjects have a poor overall outcome in terms of personal and social adjustment.
More specifically, outcome is assess in terms of repetition of self-harm and of suicide.
Between 15 and 25 percent of people who harm themselves do so again in the following year and 1–2 percent commit suicide.
Of those who harm themselves again i.e.:
- some repeat the act only once;
- some repeat it several times within a period in which there are continuing severe stressful events;
- a few repeat it many times over a long period as a habitual response to minor stressors.
The factors associated with repetition of deliberate self-harm are:
- Previous deliberate self-harm before the current episode
- Previous psychiatric treatment
- Alcohol or drug abuse
- Personality disorder
- Criminal record
- History of violence
- Low social class
- Unemployment
- Age 25–54 years
- Single, divorced, or separated
People who have deliberately harmed themselves have a much increased risk of later suicide.
In the year after the self-harm, the risk of suicide is about 1–2 per cent, that is, about 100 times the risk in the general population.
It is important to note that a non-dangerous method of self-harm does not necessarily indicate a low risk of subsequent suicide (although the risk is higher when a violent or dangerous method has been used).
Assessment:
In General, Every act of deliberate self-harm should be assessed thoroughly.
In detail, For many patients seen in primary care, the physical consequences of the act and concern about the risk of repetition will lead to hospital referral.
Besides this, All deliberate self-harm patients seen in hospital emergency departments should have a psychiatric and social assessment.
All in all, Since many patients who are medically fit do not wish to stay for specialist assessment, it is essential that all emergency department medical staff are competent to assess risk.
Steps in assessment:
- The assessment should carry out in a way that encourages patients to undertake a constructive review of their problems and of the ways they can deal with them.
- If patients can then resolve their problems in this way, they may able to do so again in the future instead of resorting to self-harm again.
When to assess:
- When patients have recovered sufficiently from the physical effects of the self-harm they should interview, if possible, where the discussion will not be overheard or interrupted.
- After a drug overdose, the first step is to determine whether consciousness is impaired.
Sources of information:
- Information should obtain also from relatives or friends, the general practitioner, and any other person (such as a social worker) already involved in the patient’s care.
Information Required:
1. What were the patient’s intentions before and at the time of the attempt ?
Patients whose behaviour suggests that they intended to die as a result of the act of self harm are at greater risk of a subsequent fatal act of self-harm.
Intent is assess by considering the following:
- Was the act planned or carried out on impulse ?
- Were precautions taken against being found ?
- Did the patient seek help after the act ?
- Was the method dangerous ?Not only should the objective risk be assessed, but also the risk anticipated by the patient, which may be different (e.g. if he believed that he had taken a lethal dose of a drug even though he had not).
- Was there a ‘final act’ such as writing a suicide note or making a will?
2. Does the patient now wish to die ?
- The interviewer should ask directly whether the patient is relieved to have recovered or wishes to die.
- If the act suggested serious suicidal intent, but the patient denies such intent, the interviewer should try to find out by tactful but thorough questioning whether there has been a genuine change of resolve.
3. What are the current problems ?
- Many patients will have experienced a mounting series of difficulties in the weeks or months leading up to the act of self-harm.
- Some of these difficulties may have resolved by the time the patient is interviewed, but if serious problems remain, the risk of a fatal repetition is greater.
- This risk is particularly great if the problems are of loneliness or ill health.
- Possible problems should review systematically, covering intimate relationships with the spouse or another person, relations with children and other relatives, employment, finance, and housing, legal problems, social isolation, bereavement, and other losses.
4. Is there any psychiatric disorder ?
- This question is answer with information obtained from the history, from a brief but systematic examination of the mental state, and also from other informants and from medical notes.
5. What are the patient’s resources ?
- These include the capacity to solve problems, material resources, and the help that others may provide.
- The best guide to future ability to solve problems is the past record of dealing with difficulties such as the loss of a job, or a broken relationship.
- The availability of help should be assessed by asking about the patient’s friends and relatives, and about support available from medical services, social workers, or voluntary agencies.
6. Is treatment required and will the patient agree to it ?
Management aims to i.e.:
- Treat any psychiatric disorder;
- Manage high suicide risk;
- Enable the patient to resolve difficulties that led to the act of self-harm;
- Deal with future crises without resorting to self-harm.
Management:
Generally, The patient is encourage to consider what steps he could take to resolve each of these problems, also to formulate a practical plan for tackling one at a time.
Furthermore, Throughout this discussion, the therapist helps the patient to do as much as possible to help himself.
At Last, When there are interpersonal problems, it is often helpful to have a joint or family discussion.
The results of treatment:
- Successful treatment of a depressive or other psychiatric disorder reduces the risk of subsequent self-harm.
- There is less strong evidence that problem solving and other psychological methods reduce repetition, although they do reduce personal and social problems.
- This lack of strong evidence may due, in part, to the methodological difficulties of randomized trials in this heterogeneous population.
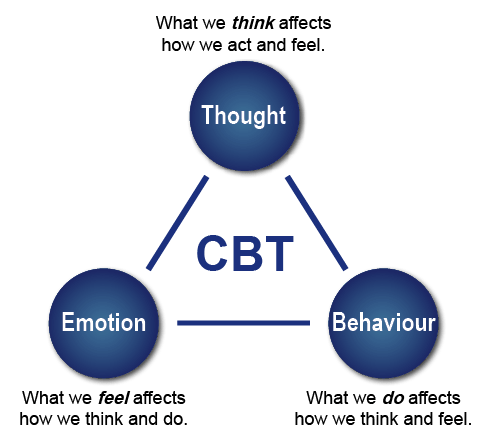
- Particular types of psychological or social problem have shown to benefit from specific treatments, such as couple therapy for problems between couples, problem solving for practical and everyday difficulties, and cognitive behaviour treatment for longstanding personal difficulties.
Management of special groups:
Certain subgroups of patients pose special management problems. In most cases, specialist advice should obtain.
Mothers of young children:
- Because there is an association between deliberate self-harm and child abuse, it is important to ask any mother with young children about her feelings towards the children, and to enquire from other informants, as well as the patient, about their welfare.
- If there is a possibility of child abuse or neglect, appropriate assessment action should be carried out.
- There is also an association between depression and infanticide.
Children and adolescents:
- Deliberate self-harm is uncommon among young children, but becomes increasingly frequent after the age of 12, especially among girls.
- The most common method is drug overdose; in only a few cases is there a threat to life.
- The motivation for self-harm in young children is difficult to determine, but it is more often to communicate distress or escape from stress than to die.
- Deliberate self-harm in children and adolescents is associate with broken homes, family psychiatric disorder, and child abuse.
- It is often precipitate by difficulties with parents, boyfriends or girlfriends, or schoolwork.
- Most children and adolescents do not repeat an act of deliberate self-harm, but an important minority do so, usually in association with severe psychosocial problems.
- These repeated acts of deliberate self-harm carry a significant risk of suicide.
- Children or adolescents who harm themselves should be assessed by a child psychiatrist.
- Treatment is not only of the young person but also of the family.
Patients who refuse assessment and treatment:
- Generally, In most countries, there is a legal power to detain those who require potentially life-saving treatment also whose competence or capacity to take an informed decision about discharge is likely to be impaired by their mental state.
- Besides this, The doctor should obtain as much information about mental state also suicidal risk as time allows.
- The patient should only be allowed to leave hospital when serious suicidal risk has been excluded.
- In taking decisions about emergency treatment, the doctor is likely to be helped by relatives, additionally; inpatient medical notes, also by telephoning the primary care doctor, social worker, or person who has been involved with the patient in the past.
- It is essential to write detailed notes and to be aware of the legal requirements about both emergency treatment and confidentiality.
Frequent repeaters:
- Some people take overdoses repeatedly, often at times of stress in circumstances that suggest that the behaviour is to either reduce tension or gain attention.
- Furthermore, These people usually have a personality disorder also many insoluble social problems.
- Although sometimes directed towards gaining attention, repeated self-harm may cause relatives to become unsympathetic or hostile, and these feelings may be shared by professional staff as their repeated efforts at help are seen to fail.
- Neither counselling nor intensive psychotherapy is effective, and management is limited to providing support.
- Sometimes a change in life circumstances is followed by improvement, but unless this happens the risk of death by suicide is high.
Deliberate self-laceration:
- It is difficult to help people who lacerate themselves repeatedly.
- They often have low self-esteem and experience extreme tension.
- Efforts should be made to increase self-esteem and to find an alternative, simple way of relieving tension, for example, by taking exercise.
- Anxiolytic drugs are seldom helpful and may produce disinhibition.
- Lastly, If drug treatment is needed to reduce tension, a phenothiazine is more likely to be effective.
Frequently Asked Questions
What is Deliberate Self-harm?
Deliberate self-harm is not usually fail suicide. Only about a quarter of those who have deliberately harmed themselves say they wished to die; most say the act was impulsive rather than premeditated.
What are the methods of Deliberate Self-harm?
- Drug Overdose
- The use of alcohol
- Self Injury
- Deeper lacerations,
- Jumping from heights
- Jumping in front of a either moving train or motor vehicle
- Shooting
- Drowning
- Burning
What are the causes of Deliberate Self-harm?
- Psychiatric disorder
- Personality disorder
- Alcohol dependence
- Predisposing social factors
- Early parental loss
- Parental neglect or abuse
- Long-term social problems: e.g. family, employment, financial
- Poor physical health
- Precipitating social factors
- Stressful life problems
How to manage the case of Deliberate Self-harm?
- Every act assessed thoroughly
- Physical consequences of the act- hospital referral
- Psychiatric also social assessment
- All emergency department medical staff are competent to assess risk
Psychiatry, Fourth Edition – Oxford Medical Publications -SRG-by John Geddes, Jonathan Price, Rebecca McKnight / Ch 9.