Phobic Disorder
Definition:
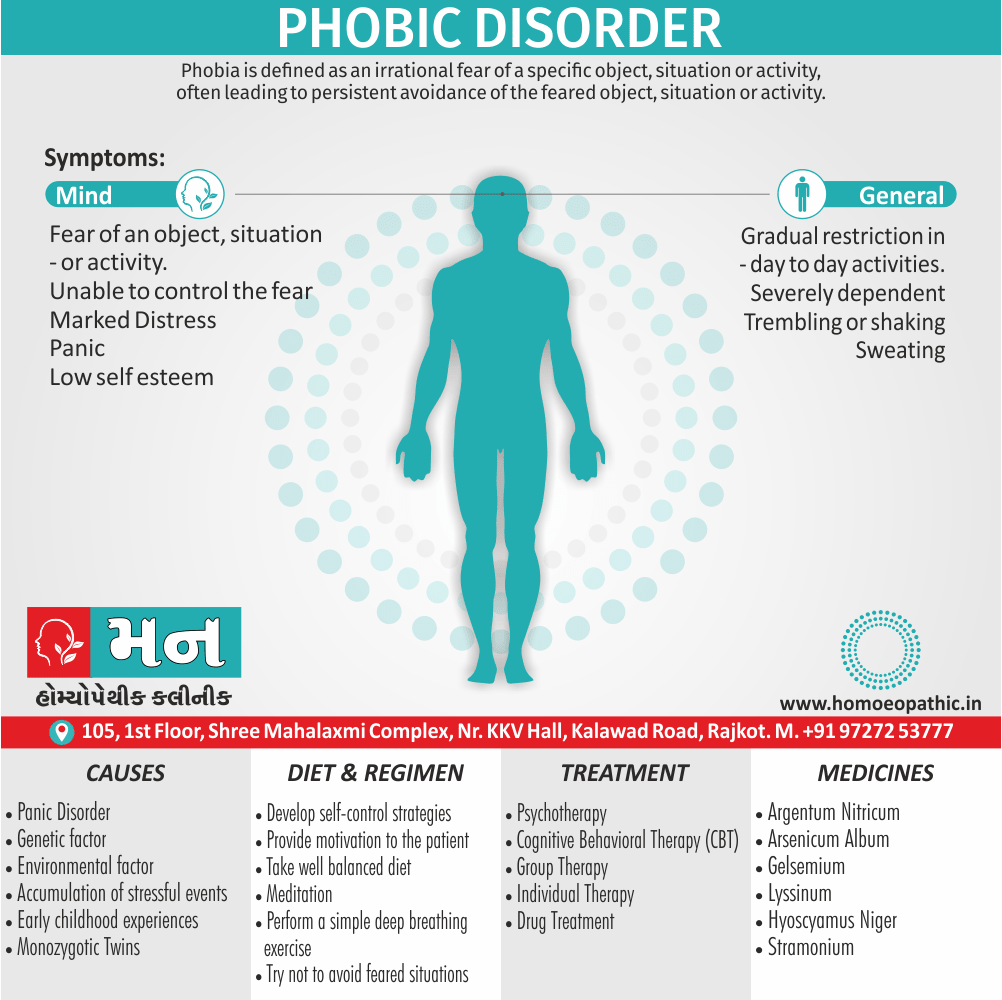
Phobia or Phobic Disorder is defined as an irrational fear of a specific object, situation or activity, often leading to persistent avoidance of the feared object, situation or activity. [2]
Some Characteristic Features of Phobic Disorder:
- Presence of the fear of an object, situation or activity.
- The fear is out of proportion to the dangerous ness perceived.
- Patient recognises the fear as irrational and unjustified (Insight is present).
- Patient is unable to control the fear and is very distressed by it.
- This leads to persistent avoidance of the particular object, situation or activity.
- Gradually, the Phobic Disorder and the phobic object become a preoccupation with the patient, resulting in marked distress and restriction of the freedom of mobility (afraid to encounter the phobic object; phobic avoidance).
Definition:
Agoraphobia is a condition in which the patient experiences anxiety in situations that are unfamiliar, from which they cannot escape, or in which they perceive they have little control. [1]
Agoraphobia is an example of irrational fear of situations. It is the commonest type of phobia encountered in clinical practice.
Women far outnumber men in suffering from agoraphobia in the Western countries.
Symptoms may include:
- It is characterised by an irrational fear of being in places away from the familiar setting of home.
- Although it was earlier thought to be a fear of open spaces only, now it includes fear of open spaces, public places, crowded places, and any other place from where there is no easy escape to a safe place.
- In fact, the patient is afraid of all the places or situations from where escape may be perceived to be difficult or help may not be available, if he suddenly develops embarrassing or incapacitating symptoms.
- These embarrassing or incapacitating symptoms are the classical symptoms of panic.
- A full-blown panic attack may occur (agoraphobia with panic disorder) or only a few symptoms (such as dizziness or tachycardia) may occur (agoraphobia without panic disorder).
- As the agoraphobia increases in severity, there is a gradual restriction in the normal day-to-day activities.
- The activities may become so severely restricted that the person becomes self-imprisoned at his home.
- One or two persons (usually close relations or friends) may be relied upon, with whom the patient can leave home.
- Hence, the patient becomes severely dependent on these phobic companion(s). [2]
Situations feared and avoided by patients with agoraphobia:
Common themes:
- Distance from home
- Crowding Confinement
- Open spaces
- Social situations
Examples:
- Public transport
- Crowded shops
- Empty streets
- School visits
- Cinemas, theatres
In both DSM-IV and ICD-10, agoraphobia is not a codable disorder on its own.
In either criteria, the diagnosis must be related to the presence or absence of panic disorder, expressed as being either panic disorder with agoraphobia (DSM-IV)/agoraphobia with panic disorder (ICD-10) or agoraphobia without a history of panic disorder.
Course and outcome:
Onset:
The median age of onset for agoraphobia is 20 years, but there are two peaks; 15–30 years and 70–80 years.
The first episode of agoraphobia often occurs while the person is away from home, waiting for public transport, or shopping in a crowded store.
Suddenly, the person develops an unexplained panic attack, and either hurries home or seeks immediate medical help.
This first episode subsides before long, but there is another when the same or similar situation is encountered again, and another hurried escape is made.
It is unusual to discover any immediate cause for the first panic attack, although some patients describe a background of problems at the time (e.g. worry about a sick child).
The development of agoraphobic symptoms late in life is often linked to physical frailty, and the fear that an accident or major medical illness will occur.
As the condition progresses, patients become increasingly dependent on the partner or other relatives for help with activities, such as shopping, that provoke anxiety.
These demands on the partner sometimes lead to arguments, and serious marital problems are common.
Co-morbidity:
The most common comorbid condition is panic attacks, but agoraphobia is also associated with other anxiety disorders, depression, and alcohol misuse disorders.
Etiology:
The cause of the first panic attack is uncertain.
It could be caused by panic disorder in which case agoraphobia is simply a variant of panic disorder.
Alternatively, the first panic attack could have another cause such as an accumulation of stressful events, in which case agoraphobia and panic disorder are separate conditions.
Differential diagnosis:
Generalized anxiety disorder i.e.:
Although this does not have the pattern of avoidance characteristic of agoraphobia. The patient usually has excessive worries about all aspects of life, not just those that fit into the common themes of distance from home, crowding, and confinement.
Social phobia i.e.:
Although agoraphobic patients feel anxious in social situations and some social phobics avoid crowded buses and shops, the overall pattern of anxiety provoking situations is different.
Simple phobias i.e.:
It may involve panic attacks, but they only occur in the presence of a specific situation or object, and do not fit into the common themes outlined above.
Depressive disorder i.e.:
Sometimes a person with longstanding agoraphobia seeks help when depressed. They will show the typical core symptoms of low mood, anhedonia, and lack of energy.
Schizophrenia i.e.:
Rarely, patients with overly suspicious delusions avoid meeting people in a way that suggests agoraphobia. If they hide the delusions, diagnosis may be difficult but a thorough history and mental state examination usually show the true diagnosis.
Treatment:
Treatment begins with the general measures
- CBT : graded-exposure therapy
- Group
- Individual
Antidepressants i.e.:
They are of value not only for their general anxiolytic effect but also because some have anti-panic effects.
SSRIs are the first line choice, with the best evidence being for fluoxetine, fluvoxamine, citalopram, and sertraline.
Their use should be combined with exposure, either as a self-help procedure or as part of cognitive behaviour therapy.
Anxiolytics i.e.:
Anxiolytics (e.g. benzodiazepines) should be avoided, except for the short-term alleviation of incapacitating symptoms or when waiting for an SSRI to take effect.
There is some evidence that the most effective treatment for agoraphobia is a combination of cognitive behaviour therapy and medication. [1]
Social Phobic Disorder:
Social phobia is incapacitating inappropriate anxiety in social situations which leads to the desire for escape or avoidance.
In the ICD-10 classification the term social phobia is preferred, whereas the DSM-IV uses the terms social phobia and social anxiety disorder interchangeably to describe the same condition. [1]
This is an example of irrational fear of activities or social interaction, characterised by an irrational fear of performing activities in the presence of other people or interacting with others.
The patient is afraid of his own actions being viewed by others critically, resulting in embarrassment or humiliation.
There is marked distress and disturbance in routine daily functioning.
Symptoms include:
- Fear of blushing (in other words, erythrophobia),
- Eating in company of others,
- Public speaking,
- Public performance (e.g. on stage),
- Participating in groups,
- Writing in public (e.g. signing a check),
- Speaking to strangers (e.g. for asking for directions),
- Dating,
- Speaking to authority,
- Urinating in a public lavatory (shy bladder). [2]
Avoidance: Sometimes the avoidance is partial; for example, entering a social group but failing to make conversation, or sitting in an inconspicuous place in the group.
Use of alcohol: Some people take alcohol to relieve anxiety, also alcohol abuse is more common among social phobics than among people with other phobias.
Low self-esteem: and perfectionism are common traits amongst those with social phobia.
Onset and Course:
The condition usually begins with an acute attack of anxiety in some public place.
Subsequently, anxiety occurs in similar places, with episodes that become gradually more severe also with increasing avoidance.
Co-morbidity:
About 80 percent of patients with social phobia will fit diagnostic criteria for another psychiatric disorder.
The most common are other anxiety disorders, depression, post-traumatic stress disorder (in other words, PTSD), and alcohol use disorders.
Etiology:
The cause of this Phobic Disorder is uncertain.
Symptoms usually start in late adolescence, a time when many young people are concerned about the impression they are making on other people.
It is possible that social phobias begin as exaggerated normal concerns, which are then increased and prolonged by thoughts that other people will be critical of any signs of anxiety.
It may be that styles of parenting and early childhood experiences influence the development of social anxiety.
Patients with social anxiety often remember their mother being fearful in social situations, and frequently describe their parents as overprotective.
Genetics certainly play a role in the aetiology of social anxiety disorder, but the extent of this is currently unknown.
Concordance rates for monozygotic twins (25 percent) are higher than for dizygotic twins (15 percent), and it known (but not quantified) that first-degree relatives of those with the disorder have a greater risk of developing it than the general population.
Differential diagnosis:
Generalized anxiety disorder:
Social phobia distinguish by the pattern of situations in which anxiety occurs.
Depressive disorder:
This Phobic Disorder distinguish by the pattern of situations and the absence of the core symptoms of low mood, anhedonia, and loss of energy.
Sometimes people who have previously coped with social phobia seek help when they become depressed.
Schizophrenia:
Occasionally, patients with schizophrenia are anxious in, and avoid, social situations because of overly suspicious delusions.
Anxious/avoidant personality disorder:
It is characterized by lifelong shyness and lack of self-confidence, may closely resemble social phobia.
However, personality disorder starts at a younger age and develops more gradually than social phobia.
Social inadequacy:
It is a primary lack of social skills with secondary anxiety. People with social phobia possess these social skills but cannot use them when they are anxious.
Treatment:
Antidepressant medication:
The best evidence is for the use of one of the SSRIs.
Paroxetine, fluvoxamine, escitalopram, and sertraline have reported to be effective in social phobia in the short term although the long-term benefits are less certain.
A second-line option is the SNRI venlafaxine, which is of similar efficacy to SSRIs but has a poorer side-effect profile.
Traditionally, the monoamine oxidase inhibitors (e.g. moclobemide) use for social anxiety, but the strict dietary restrictions needed to use them safely combined with adverse side effects mean their use is only justified when other medications prove ineffective.
While taking any antidepressant medication, patients should advise to practise exposure to situations that they have previously avoided.
Anxiolytic medication:
It provides immediate short-term relief, for example to help the patient deal with an important professional or social situation before more lasting treatment has taken effect.
However, anxiolytics should not use regularly because of the risk of dependence.
Beta-adrenergic antagonists (e.g. propranolol) are used occasionally to control tremor and palpitations unresponsive to anxiolytic treatment, but have not been shown to be better than placebo at controlling social anxiety when used on a regular basis.
A person with simple Phobic Disorder is inappropriately anxious in the presence of a particular object or situation, or when anticipating this encounter, and has the urge to avoid the object or situation.
Anticipatory anxiety is often severe; for example, a person who fears storms may become extremely anxious when there are only black clouds, which might precede a storm.
A list of common phobias is include:
Objects that induce anxiety:
- Blood (haematophobia)
- Excretion
- Vomit or vomiting (emetophobia)
- Needles or injections (trypanophobia)
- Animals (zoophobia),e.g. Spiders (arachnophobia), Snakes (ophidiophobia)
Situations that induce anxiety:
- Dentists (5% of adults; may lead to poor dentition)
- Darkness (scotophobia)
- Elevators
- Storms or thunder
- Flying or airplanes [1]
- Acrophobia (fear of high places),
- Xenophobia (fear of strangers),
- Algophobia (fear of pain),
- Claustrophobia (fear of closed places).
Specific phobia is characterised by an irrational fear of a specified object or situation.
Anticipatory anxiety leads to persistent avoidant behaviour, while confrontation with the avoided object or situation leads to panic attacks.
Gradually, the phobia usually spreads to other objects and situations.
The disorder is diagnosed only if there is marked distress and/or disturbance in daily functioning, in addition to fear and avoidance of the specified object or situation. [2]
Co-morbidity:
Of individuals with a simple phobia, 83.4 percent will meet criteria for another psychiatric diagnosis at some time in their life. These are most commonly other anxiety disorders or depression.
Etiology:
Most of the simple phobias of adult life begin in childhood when simple phobias are extremely common.
Why most childhood phobias disappear and a few persist into adult life is not known, except that the most severe phobias are more likely to do so.
Simple phobias that begin in adult life often develop after a very frightening experience; for example, a phobia of horses following a dangerous encounter with a bolting horse.
Phobias are due to classical conditioning, the individual reinforcing a learned behaviour after a negative experience with an object or situation.
The most important behaviour that maintains the fear and makes it hard to eliminate is avoidance.
The concordance rates for animal phobias in monozygotic and dizygotic twins are 25 percent and 11 percent, respectively, but there are no data available for most other phobias.
Differential Diagnosis:
Some patients with long-standing simple phobias seek help when an unrelated depressive disorder makes them less able to tolerate the phobic symptoms.
Apart from this association, simple phobia is seldom mistaken for another disorder.
Treatment:
It is worth noting that the majority of patients need no treatment beyond sensible advice unless the phobia is having a significant impact on their well-being.
Cognitive behaviour therapy:
The treatment of choice for simple phobia is graded exposure therapy, which is a structured programme aiming to gradually reintroduce the patient to the phobic situation in a supportive manner.
Medication:
Patients sometimes ask for immediate relief of symptoms when a long-standing phobia makes it difficult to fulfil a forthcoming important engagement (e.g. a claustrophobic person who requires an urgent MRI scan).
In such circumstances, a benzodiazepine can be used, but in the short term only the use of sedative medication in such circumstances is another way of avoiding the feared stimulus.
It is not usually appropriate to prescribe an antidepressant, as the symptoms of simple phobia are by definition very intermittent. [1]
Homeopathic Medicines for Phobic Disorder:
Fear of death (Thanatophobia)
Aconite – Homeopathic Medicine for Fear of Death with Anxiety.
Aconite is a homeopathic medicine that use to treat the fear of death coupled with anxiety. The person may fear death and believe that they may die soon, going so far as to predict the day of demise.
Arsenicum Album – Homeopathic Medicine for Fear of Death with Restlessness.
Arsenicum Album homeopathic medicine use to treat the fear of death accompanied by restlessness. The affected person does not feel the need to take any medication and may change places continuously.
Homeopathic Medicine for Fear of Heights (Acrophobia):
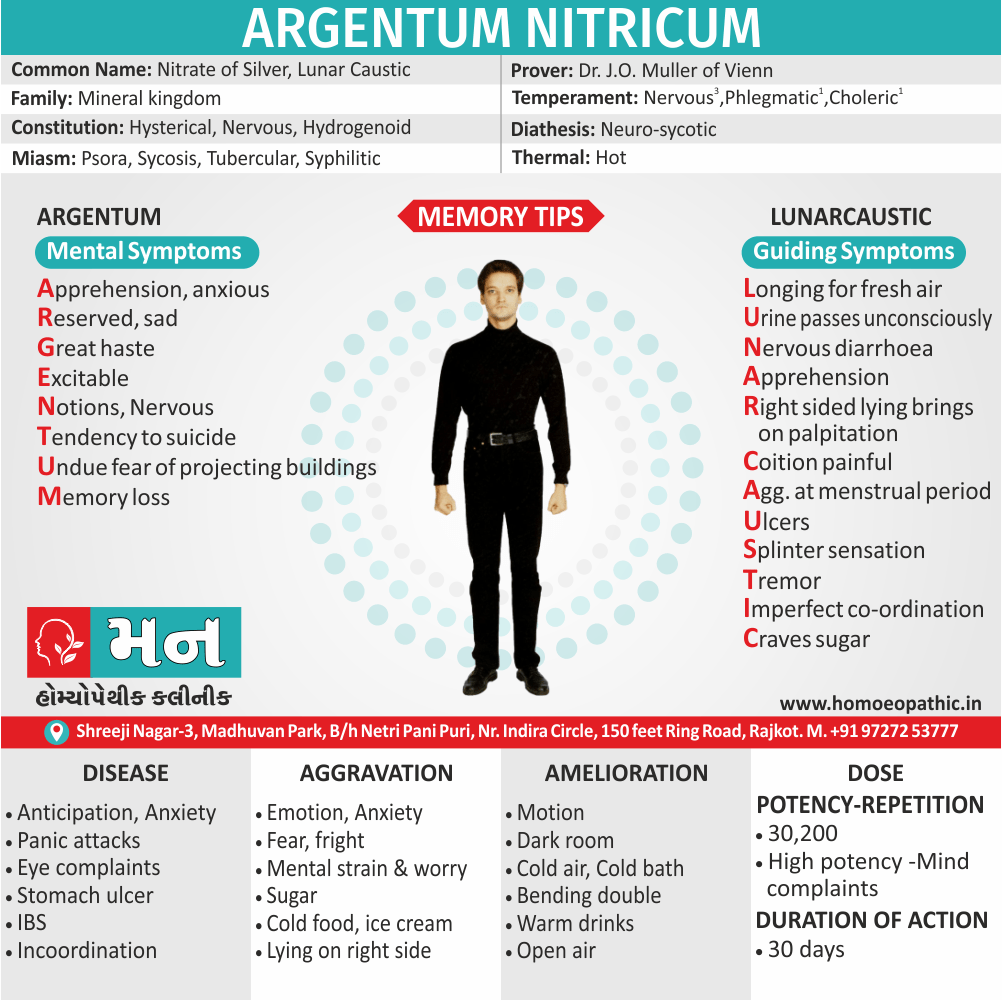
Argentum Nitricum – Homeopathic Medicine for Fear of Height.
Argentum Nitricum homeopathic medicine use to treat the fear of height and of flying in airplanes.
The person fears the projecting corners of buildings; the sight of high buildings makes the person giddy and may cause him or her to stagger.
A feeling of having the buildings on both sides of the street closing in and crushing upon the person is prevalent.
Homeopathic Medicines for Fear of Closed Places (Claustrophobia):
Stramonium – Homeopathic medicine for Fear with Desire to Escape.
Stramonium homeopathic medicine use to treat the fear of closed places with a desire to escape. The affected person may get anxiety when going through a tunnel or similar closed space.
Pulsatilla – Homeopathic Medicine for Fear with Desire for Open Spaces.
Pulsatilla homeopathic medicine used to treat a fear of close spaces coupled with the desire to seek open air.
Homeopathic Medicines for Fear of Open Places (Agoraphobia):
Gelsemium – Homeopathic Medicine for Stage Fright.
Gelsemium homeopathic medicine use to treat the fear of open places, especially stage fright. The affected person has a nervous dread of appearing in public.
Phosphorus – Homeopathic Medicine for Fear of Mishappening.
Phosphorus homeopathic medicine use to treat the fear of open places wherein the person fears that something terrible will happen.
Homeopathic Medicines for Fear of Water (Hydrophobia):
Lyssinum – Homeopathic Medicine for Fear of Water with Anxiety.
Lyssinum homeopathic medicine used to treat fear of water couple with anxiety, where a person wants to drink water but is unable to do so. Irritability on hearing the sound of water or looking at it is present, and the person gets convulsions on thinking of water or fluids.
Hyoscyamus – Homeopathic Medicine for Fear with Delirium.
Hyoscyamus homeopathic medicine use to treat the fear of eating or drinking coupled with delirium. The person develops anxiety on hearing the sound of running water.
Homeopathic Medicines for Fear of failure (Atychiphobia):
Lycopodium – Homeopathic Medicine for Fear and Weak Memory.
Lycopodium homeopathic medicine use to treat the fear of failure with weak memory. Additionally, The person has a strong aversion to undertaking new challenges and may feel unable to reach a destination.
Aurum Metallicum – Homeopathic Medicine for Fear with Hopelessness.
Aurum Metallicum homeopathic medicine use to treat the fear of failure with marked hopelessness.
In detail, The person experiences acute mental depression, the future looks bleak, and a feeling of being unfit or undeserving may prevail.
Homeopathic Medicines for Fear of Sex (Intimacy)
Kreosote – Homeopathic Medicine for Fear of Intimacy.
Kreosote a homeopathic medicine especially use to treat the fear of sex also intimacy in women.
Staphysagria – Homeopathic Medicine for Fear with Suppressed Desire.
Generally, Staphysagria a homeopathic medicine use to treat the fear of sex with suppressed sexual desire. The tendency to fear sex may sprout from a feeling of being out of control, or with a history of rape or sexual abuse.
Homeopathic Medicines for Fear of Disease
Kali Arsenicum – Homeopathic Medicine for Fear of Life-threatening Disease.
Kali Arsenicum a homeopathic medicine use to treat the fear of contracting a life-threatening disease or anxiety about health, especially on going to bed.
This medicine indicate in cases where there is a fear of having a stroke, heart disease or high blood pressure.
Agaricus – Homeopathic Medicine for Fear of Cancer.
Agaricus a homeopathic medicine use to treat the fear of disease, especially cancer. The affected person may pre-occupy with thoughts of death, dying and graveyards. [3]
Frequently Asked Questions
What is Phobic Disorder?
Phobia or Phobic Disorder define as an irrational fear of a specific object, situation or activity, often leading to persistent avoidance of the feared object, situation or activity.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Phobic Disorder?
- Aconite
- Arsenicum Album
- Argentum Nitricum
- Stramonium
- Pulsatilla
- Gelsemium
- Phosphorus
- Lyssinum
What are the characteristic features of Phobic Disorder?
- Fear of an object, situation or activity.
- Fear is out of proportion to the dangerous
- Recognises the fear as irrational and unjustified
- Unable to control the fear
- Persistent avoidance of the particular object, situation or activity.
- Marked distress and restriction of the freedom
What are the types of Phobic Disorder?
- Agoraphobia
- Social phobia
- Specific (Simple) phobia
References of Phobic Disorder:
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 24.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 8.
- https://www.drhomeo.com/fear/homeopathy-for-fears-and-phobias/
Definition:
Phobia or Phobic Disorder is defined as an irrational fear of a specific object, situation or activity, often leading to persistent avoidance of the feared object, situation or activity. [2]
Overview
Epidemiology
Causes
Risk Factors
Pathogenesis
Pathophysiology
Types
1. Agoraphobia
2. Social Phobia
3. Simple Phobia
Clinical Features
Sign & Symptoms
Clinical Examination
Diagnosis
Differential Diagnosis
Complications
Investigations
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Terminology
References
FAQ
Also Search As
Overview
Some Characteristic Features of Phobic Disorder:
- Presence of the fear of an object, situation or activity.
- The fear is out of proportion to the dangerous ness perceived.
- Patient recognises the fear as irrational and unjustified (Insight is present).
- Patient is unable to control the fear and is very distressed by it.
- This leads to persistent avoidance of the particular object, situation or activity.
- Gradually, the Phobic Disorder and the phobic object become a preoccupation with the patient, resulting in marked distress and restriction of the freedom of mobility (afraid to encounter the phobic object; phobic avoidance).
Epidemiology
Indian epidemiology then other
Causes
This refers to the initiating factors that trigger a disease process.
- Examples of causes include:
- Pathogens: Viruses, bacteria, fungi, parasites (infectious diseases)
- Genetic mutations: Inherited or spontaneous changes in genes (genetic diseases)
- Environmental factors: Toxins, radiation, nutritional deficiencies
- Lifestyle choices: Smoking, unhealthy diet, lack of exercise (contributing factors)
Risk Factors
Risk factors are things that make you more likely to develop a disease in the first place.
Pathogenesis
Pathogenesis refers to the development of a disease. It’s the story of how a disease gets started and progresses.
This is the entire journey of a disease, encompassing the cause but going beyond it.
Pathophysiology
Pathophysiology, on the other hand, focuses on the functional changes that occur in the body due to the disease. It explains how the disease disrupts normal physiological processes and how this disruption leads to the signs and symptoms we see.
Imagine a car accident. Pathogenesis would be like understanding how the accident happened – what caused it, the sequence of events (e.g., one car ran a red light, then hit another car). Pathophysiology would be like understanding the damage caused by the accident – the bent fenders, deployed airbags, and any injuries to the passengers.
In simpler terms, pathogenesis is about the "why" of a disease, while pathophysiology is about the "how" of the disease’s effects.
Types
1. Agoraphobia
Definition:
Agoraphobia is a condition in which the patient experiences anxiety in situations that are unfamiliar, from which they cannot escape, or in which they perceive they have little control. [1]
Agoraphobia is an example of irrational fear of situations. It is the commonest type of phobia encountered in clinical practice.
Women far outnumber men in suffering from agoraphobia in the Western countries.
Symptoms may include:
- It is characterised by an irrational fear of being in places away from the familiar setting of home.
- Although it was earlier thought to be a fear of open spaces only, now it includes fear of open spaces, public places, crowded places, and any other place from where there is no easy escape to a safe place.
- In fact, the patient is afraid of all the places or situations from where escape may be perceived to be difficult or help may not be available, if he suddenly develops embarrassing or incapacitating symptoms.
- These embarrassing or incapacitating symptoms are the classical symptoms of panic.
- A full-blown panic attack may occur (agoraphobia with panic disorder) or only a few symptoms (such as dizziness or tachycardia) may occur (agoraphobia without panic disorder).
- As the agoraphobia increases in severity, there is a gradual restriction in the normal day-to-day activities.
- The activities may become so severely restricted that the person becomes self-imprisoned at his home.
- One or two persons (usually close relations or friends) may be relied upon, with whom the patient can leave home.
- Hence, the patient becomes severely dependent on these phobic companion(s). [2]
Situations feared and avoided by patients with agoraphobia:
Common themes:
- Distance from home
- Crowding Confinement
- Open spaces
- Social situations
Examples:
- Public transport
- Crowded shops
- Empty streets
- School visits
- Cinemas, theatres
In both DSM-IV and ICD-10, agoraphobia is not a codable disorder on its own.
In either criteria, the diagnosis must be related to the presence or absence of panic disorder, expressed as being either panic disorder with agoraphobia (DSM-IV)/agoraphobia with panic disorder (ICD-10) or agoraphobia without a history of panic disorder.
Course and outcome:
Onset:
The median age of onset for agoraphobia is 20 years, but there are two peaks; 15–30 years and 70–80 years.
The first episode of agoraphobia often occurs while the person is away from home, waiting for public transport, or shopping in a crowded store.
Suddenly, the person develops an unexplained panic attack, and either hurries home or seeks immediate medical help.
This first episode subsides before long, but there is another when the same or similar situation is encountered again, and another hurried escape is made.
It is unusual to discover any immediate cause for the first panic attack, although some patients describe a background of problems at the time (e.g. worry about a sick child).
The development of agoraphobic symptoms late in life is often linked to physical frailty, and the fear that an accident or major medical illness will occur.
As the condition progresses, patients become increasingly dependent on the partner or other relatives for help with activities, such as shopping, that provoke anxiety.
These demands on the partner sometimes lead to arguments, and serious marital problems are common.
Co-morbidity:
The most common comorbid condition is panic attacks, but agoraphobia is also associated with other anxiety disorders, depression, and alcohol misuse disorders.
Etiology:
The cause of the first panic attack is uncertain.
It could be caused by panic disorder in which case agoraphobia is simply a variant of panic disorder.
Alternatively, the first panic attack could have another cause such as an accumulation of stressful events, in which case agoraphobia and panic disorder are separate conditions.
Differential diagnosis:
Generalized anxiety disorder i.e.:
Although this does not have the pattern of avoidance characteristic of agoraphobia. The patient usually has excessive worries about all aspects of life, not just those that fit into the common themes of distance from home, crowding, and confinement.
Social phobia i.e.:
Although agoraphobic patients feel anxious in social situations and some social phobics avoid crowded buses and shops, the overall pattern of anxiety provoking situations is different.
Simple phobias i.e.:
It may involve panic attacks, but they only occur in the presence of a specific situation or object, and do not fit into the common themes outlined above.
Depressive disorder i.e.:
Sometimes a person with longstanding agoraphobia seeks help when depressed. They will show the typical core symptoms of low mood, anhedonia, and lack of energy.
Schizophrenia i.e.:
Rarely, patients with overly suspicious delusions avoid meeting people in a way that suggests agoraphobia. If they hide the delusions, diagnosis may be difficult but a thorough history and mental state examination usually show the true diagnosis.
Treatment:
Treatment begins with the general measures
- CBT : graded-exposure therapy
- Group
- Individual
Antidepressants i.e.:
They are of value not only for their general anxiolytic effect but also because some have anti-panic effects.
SSRIs are the first line choice, with the best evidence being for fluoxetine, fluvoxamine, citalopram, and sertraline.
Their use should be combined with exposure, either as a self-help procedure or as part of cognitive behaviour therapy.
Anxiolytics i.e.:
Anxiolytics (e.g. benzodiazepines) should be avoided, except for the short-term alleviation of incapacitating symptoms or when waiting for an SSRI to take effect.
There is some evidence that the most effective treatment for agoraphobia is a combination of cognitive behaviour therapy and medication. [1]
2. Social Phobia
Social Phobic Disorder:
Social phobia is incapacitating inappropriate anxiety in social situations which leads to the desire for escape or avoidance.
In the ICD-10 classification the term social phobia is preferred, whereas the DSM-IV uses the terms social phobia and social anxiety disorder interchangeably to describe the same condition. [1]
This is an example of irrational fear of activities or social interaction, characterised by an irrational fear of performing activities in the presence of other people or interacting with others.
The patient is afraid of his own actions being viewed by others critically, resulting in embarrassment or humiliation.
There is marked distress and disturbance in routine daily functioning.
Symptoms include:
- Fear of blushing (in other words, erythrophobia),
- Eating in company of others,
- Public speaking,
- Public performance (e.g. on stage),
- Participating in groups,
- Writing in public (e.g. signing a check),
- Speaking to strangers (e.g. for asking for directions),
- Dating,
- Speaking to authority,
- Urinating in a public lavatory (shy bladder). [2]
Avoidance: Sometimes the avoidance is partial; for example, entering a social group but failing to make conversation, or sitting in an inconspicuous place in the group.
Use of alcohol: Some people take alcohol to relieve anxiety, also alcohol abuse is more common among social phobics than among people with other phobias.
Low self-esteem: and perfectionism are common traits amongst those with social phobia.
Onset and Course:
The condition usually begins with an acute attack of anxiety in some public place.
Subsequently, anxiety occurs in similar places, with episodes that become gradually more severe also with increasing avoidance.
Co-morbidity:
About 80 percent of patients with social phobia will fit diagnostic criteria for another psychiatric disorder.
The most common are other anxiety disorders, depression, post-traumatic stress disorder (in other words, PTSD), and alcohol use disorders.
Etiology:
The cause of this Phobic Disorder is uncertain.
Symptoms usually start in late adolescence, a time when many young people are concerned about the impression they are making on other people.
It is possible that social phobias begin as exaggerated normal concerns, which are then increased and prolonged by thoughts that other people will be critical of any signs of anxiety.
It may be that styles of parenting and early childhood experiences influence the development of social anxiety.
Patients with social anxiety often remember their mother being fearful in social situations, and frequently describe their parents as overprotective.
Genetics certainly play a role in the aetiology of social anxiety disorder, but the extent of this is currently unknown.
Concordance rates for monozygotic twins (25 percent) are higher than for dizygotic twins (15 percent), and it known (but not quantified) that first-degree relatives of those with the disorder have a greater risk of developing it than the general population.
Differential diagnosis:
Generalized anxiety disorder:
Social phobia distinguish by the pattern of situations in which anxiety occurs.
Depressive disorder:
This Phobic Disorder distinguish by the pattern of situations and the absence of the core symptoms of low mood, anhedonia, and loss of energy.
Sometimes people who have previously coped with social phobia seek help when they become depressed.
Schizophrenia:
Occasionally, patients with schizophrenia are anxious in, and avoid, social situations because of overly suspicious delusions.
Anxious/avoidant personality disorder:
It is characterized by lifelong shyness and lack of self-confidence, may closely resemble social phobia.
However, personality disorder starts at a younger age and develops more gradually than social phobia.
Social inadequacy:
It is a primary lack of social skills with secondary anxiety. People with social phobia possess these social skills but cannot use them when they are anxious.
Treatment:
Antidepressant medication:
The best evidence is for the use of one of the SSRIs.
Paroxetine, fluvoxamine, escitalopram, and sertraline have reported to be effective in social phobia in the short term although the long-term benefits are less certain.
A second-line option is the SNRI venlafaxine, which is of similar efficacy to SSRIs but has a poorer side-effect profile.
Traditionally, the monoamine oxidase inhibitors (e.g. moclobemide) use for social anxiety, but the strict dietary restrictions needed to use them safely combined with adverse side effects mean their use is only justified when other medications prove ineffective.
While taking any antidepressant medication, patients should advise to practise exposure to situations that they have previously avoided.
Anxiolytic medication:
It provides immediate short-term relief, for example to help the patient deal with an important professional or social situation before more lasting treatment has taken effect.
However, anxiolytics should not use regularly because of the risk of dependence.
Beta-adrenergic antagonists (e.g. propranolol) are used occasionally to control tremor and palpitations unresponsive to anxiolytic treatment, but have not been shown to be better than placebo at controlling social anxiety when used on a regular basis.
3. Simple Phobia
A person with simple Phobic Disorder is inappropriately anxious in the presence of a particular object or situation, or when anticipating this encounter, and has the urge to avoid the object or situation.
Anticipatory anxiety is often severe; for example, a person who fears storms may become extremely anxious when there are only black clouds, which might precede a storm.
A list of common phobias is include:
Objects that induce anxiety:
- Blood (haematophobia)
- Excretion
- Vomit or vomiting (emetophobia)
- Needles or injections (trypanophobia)
- Animals (zoophobia),e.g. Spiders (arachnophobia), Snakes (ophidiophobia)
Situations that induce anxiety:
- Dentists (5% of adults; may lead to poor dentition)
- Darkness (scotophobia)
- Elevators
- Storms or thunder
- Flying or airplanes [1]
- Acrophobia (fear of high places),
- Xenophobia (fear of strangers),
- Algophobia (fear of pain),
- Claustrophobia (fear of closed places).
Specific phobia is characterised by an irrational fear of a specified object or situation.
Anticipatory anxiety leads to persistent avoidant behaviour, while confrontation with the avoided object or situation leads to panic attacks.
Gradually, the phobia usually spreads to other objects and situations.
The disorder is diagnosed only if there is marked distress and/or disturbance in daily functioning, in addition to fear and avoidance of the specified object or situation. [2]
Co-morbidity:
Of individuals with a simple phobia, 83.4 percent will meet criteria for another psychiatric diagnosis at some time in their life. These are most commonly other anxiety disorders or depression.
Etiology:
Most of the simple phobias of adult life begin in childhood when simple phobias are extremely common.
Why most childhood phobias disappear and a few persist into adult life is not known, except that the most severe phobias are more likely to do so.
Simple phobias that begin in adult life often develop after a very frightening experience; for example, a phobia of horses following a dangerous encounter with a bolting horse.
Phobias are due to classical conditioning, the individual reinforcing a learned behaviour after a negative experience with an object or situation.
The most important behaviour that maintains the fear and makes it hard to eliminate is avoidance.
The concordance rates for animal phobias in monozygotic and dizygotic twins are 25 percent and 11 percent, respectively, but there are no data available for most other phobias.
Differential Diagnosis:
Some patients with long-standing simple phobias seek help when an unrelated depressive disorder makes them less able to tolerate the phobic symptoms.
Apart from this association, simple phobia is seldom mistaken for another disorder.
Treatment:
It is worth noting that the majority of patients need no treatment beyond sensible advice unless the phobia is having a significant impact on their well-being.
Cognitive behaviour therapy:
The treatment of choice for simple phobia is graded exposure therapy, which is a structured programme aiming to gradually reintroduce the patient to the phobic situation in a supportive manner.
Medication:
Patients sometimes ask for immediate relief of symptoms when a long-standing phobia makes it difficult to fulfil a forthcoming important engagement (e.g. a claustrophobic person who requires an urgent MRI scan).
In such circumstances, a benzodiazepine can be used, but in the short term only the use of sedative medication in such circumstances is another way of avoiding the feared stimulus.
It is not usually appropriate to prescribe an antidepressant, as the symptoms of simple phobia are by definition very intermittent. [1]
Clinical Features
Tab Content
Sign & Symptoms
Tab Content
Clinical Examination
Tab Content
Diagnosis
Tab Content
Differential Diagnosis
Complications
Complications are what happen after you have a disease. They are the negative consequences of the disease process.
Investigations
Tab Content
Treatment
Tab Content
Prevention
Tab Content
Homeopathic Treatment
Homeopathic Medicines for Phobic Disorder:
Fear of death (Thanatophobia)
Aconite – Homeopathic Medicine for Fear of Death with Anxiety.
Aconite is a homeopathic medicine that use to treat the fear of death coupled with anxiety. The person may fear death and believe that they may die soon, going so far as to predict the day of demise.
Arsenicum Album – Homeopathic Medicine for Fear of Death with Restlessness.
Arsenicum Album homeopathic medicine use to treat the fear of death accompanied by restlessness. The affected person does not feel the need to take any medication and may change places continuously.
Homeopathic Medicine for Fear of Heights (Acrophobia):
Argentum Nitricum – Homeopathic Medicine for Fear of Height.
Argentum Nitricum homeopathic medicine use to treat the fear of height and of flying in airplanes.
The person fears the projecting corners of buildings; the sight of high buildings makes the person giddy and may cause him or her to stagger.
A feeling of having the buildings on both sides of the street closing in and crushing upon the person is prevalent.
Homeopathic Medicines for Fear of Closed Places (Claustrophobia):
Stramonium – Homeopathic medicine for Fear with Desire to Escape.
Stramonium homeopathic medicine use to treat the fear of closed places with a desire to escape. The affected person may get anxiety when going through a tunnel or similar closed space.
Pulsatilla – Homeopathic Medicine for Fear with Desire for Open Spaces.
Pulsatilla homeopathic medicine used to treat a fear of close spaces coupled with the desire to seek open air.
Homeopathic Medicines for Fear of Open Places (Agoraphobia):
Gelsemium – Homeopathic Medicine for Stage Fright.
Gelsemium homeopathic medicine use to treat the fear of open places, especially stage fright. The affected person has a nervous dread of appearing in public.
Phosphorus – Homeopathic Medicine for Fear of Mishappening.
Phosphorus homeopathic medicine use to treat the fear of open places wherein the person fears that something terrible will happen.
Homeopathic Medicines for Fear of Water (Hydrophobia):
Lyssinum – Homeopathic Medicine for Fear of Water with Anxiety.
Lyssinum homeopathic medicine used to treat fear of water couple with anxiety, where a person wants to drink water but is unable to do so. Irritability on hearing the sound of water or looking at it is present, and the person gets convulsions on thinking of water or fluids.
Hyoscyamus – Homeopathic Medicine for Fear with Delirium.
Hyoscyamus homeopathic medicine use to treat the fear of eating or drinking coupled with delirium. The person develops anxiety on hearing the sound of running water.
Homeopathic Medicines for Fear of failure (Atychiphobia):
Lycopodium – Homeopathic Medicine for Fear and Weak Memory.
Lycopodium homeopathic medicine use to treat the fear of failure with weak memory. Additionally, The person has a strong aversion to undertaking new challenges and may feel unable to reach a destination.
Aurum Metallicum – Homeopathic Medicine for Fear with Hopelessness.
Aurum Metallicum homeopathic medicine use to treat the fear of failure with marked hopelessness.
In detail, The person experiences acute mental depression, the future looks bleak, and a feeling of being unfit or undeserving may prevail.
Homeopathic Medicines for Fear of Sex (Intimacy)
Kreosote – Homeopathic Medicine for Fear of Intimacy.
Kreosote a homeopathic medicine especially use to treat the fear of sex also intimacy in women.
Staphysagria – Homeopathic Medicine for Fear with Suppressed Desire.
Generally, Staphysagria a homeopathic medicine use to treat the fear of sex with suppressed sexual desire. The tendency to fear sex may sprout from a feeling of being out of control, or with a history of rape or sexual abuse.
Homeopathic Medicines for Fear of Disease
Kali Arsenicum – Homeopathic Medicine for Fear of Life-threatening Disease.
Kali Arsenicum a homeopathic medicine use to treat the fear of contracting a life-threatening disease or anxiety about health, especially on going to bed.
This medicine indicate in cases where there is a fear of having a stroke, heart disease or high blood pressure.
Agaricus – Homeopathic Medicine for Fear of Cancer.
Agaricus a homeopathic medicine use to treat the fear of disease, especially cancer. The affected person may pre-occupy with thoughts of death, dying and graveyards. [3]
Diet & Regimen
Do’s and Dont’s
Tab Content
Terminology
Tab Content
References
References of Phobic Disorder:
- Psychiatry, Fourth Edition- Oxford Medical Publications – SRG- by Geddes, Jonathan Price, Rebecca McKnight / Ch 24.
- A Short Textbook of Psychiatry by Niraj Ahuja / Ch 8.
- https://www.drhomeo.com/fear/homeopathy-for-fears-and-phobias/
FAQ
Frequently Asked Questions
What is Phobic Disorder?
Phobia or Phobic Disorder define as an irrational fear of a specific object, situation or activity, often leading to persistent avoidance of the feared object, situation or activity.
Homeopathic Medicines used by Homeopathic Doctors in treatment of Phobic Disorder?
- Aconite
- Arsenicum Album
- Argentum Nitricum
- Stramonium
- Pulsatilla
- Gelsemium
- Phosphorus
- Lyssinum
What are the characteristic features of Phobic Disorder?
- Fear of an object, situation or activity.
- Fear is out of proportion to the dangerous
- Recognises the fear as irrational and unjustified
- Unable to control the fear
- Persistent avoidance of the particular object, situation or activity.
- Marked distress and restriction of the freedom
What are the types of Phobic Disorder?
- Agoraphobia
- Social phobia
- Specific (Simple) phobia
Also Search As
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
How can I find reputable homeopathy clinics or homeopathic doctors in my area?
You can found Homeopathic Clinic For XXXX by searching for
Specific city Examples are
You can also search for near you Examples are