Organic Mental Disorders:
In Organic Mental Disorders, it is assumed that all psychological and behavioural processes, whether normal or abnormal, are a result of normal or deranged brain function. A rational corollary would be that all psychiatric disorders are due to abnormal brain functioning and are therefore organic. However, this would be a gross oversimplification.
Types of Organic Mental Disorders:
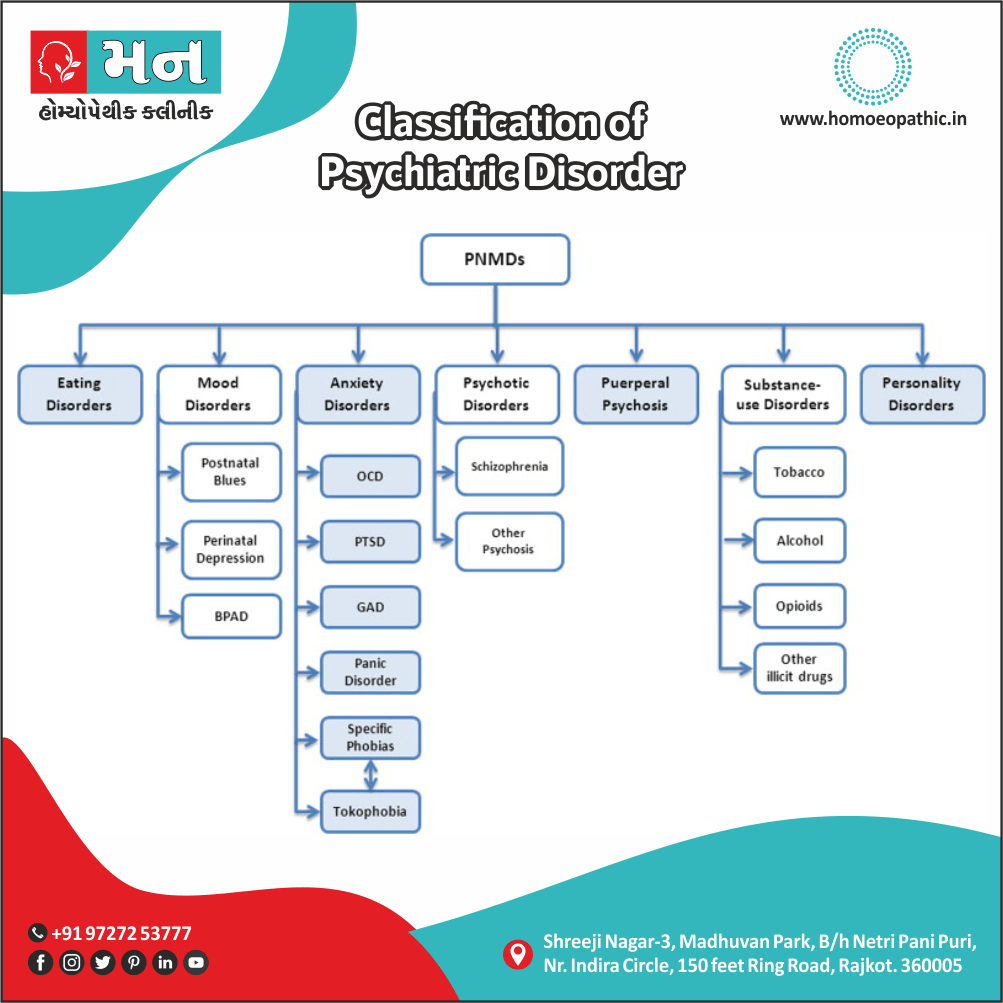
According to our present knowledge, there are broadly three types of psychiatric disorders:
- Those due to a known organic cause.
- Those in whose causation an organic factor has not yet been found or proven.
- Those primarily due to unpredictable social factors.
Only disorders with a known organic cause are called organic mental disorders. Thus, organic mental
disorders are behavioural or psychological disorders associated with transient or permanent brain dysfunction and include only those mental and behavioural disorders that are due to demonstrable cerebral disease or disorder, either primary (primary brain pathology) or secondary (brain dysfunction due to systemic diseases). The use of term organic here does not imply that other psychiatric disorders are ‘non-organic’ in the sense of having no biological basis. It simply means that the organic mental disorders have a demonstrable and independently diagnosable cerebral disease or disorder, unlike other psychiatric disorders that do not at present.
Since organic brain illness can mimic any psychiatric disorder, especially in the initial stages, organic mental disorder should be the first consideration in evaluating a patient with any psychological or behavioural clinical syndrome. The presence of following features requires a high index of suspicion for an organic mental disorder (or what is loosely called as organicity):
- First episode.
- Sudden onset.
- Older age of onset.
- History of drug and/or alcohol use disorder.
- Concurrent medical or neurological illness.
- Neurological symptoms or signs, such as seizures, impairment of consciousness, head injury, sensory or motor disturbance.
- Presence of confusion, disorientation, memory impairment or soft neurological signs.
- Prominent visual or other non-auditory (e.g. olfactory, gustatory or tactile) hallucinations.
These disorders can be broadly sub-categorised into the following categories:
Other Classification of Organic Mental Disorders:
International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version for ;2016
Chapter V
Mental and behavioural disorders
(F00-F99)
Organic, including symptomatic, mental disorders
(F00-F09)
- This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable etiology in cerebral disease, brain injury, or other insult leading to cerebral dysfunction. Additionally; The dysfunction may be primary, as in diseases, injuries, and insults that affect the brain directly also selectively; or secondary, as in systemic diseases and disorders that attack the brain only as one of the multiple organs or systems of the body that are involved.
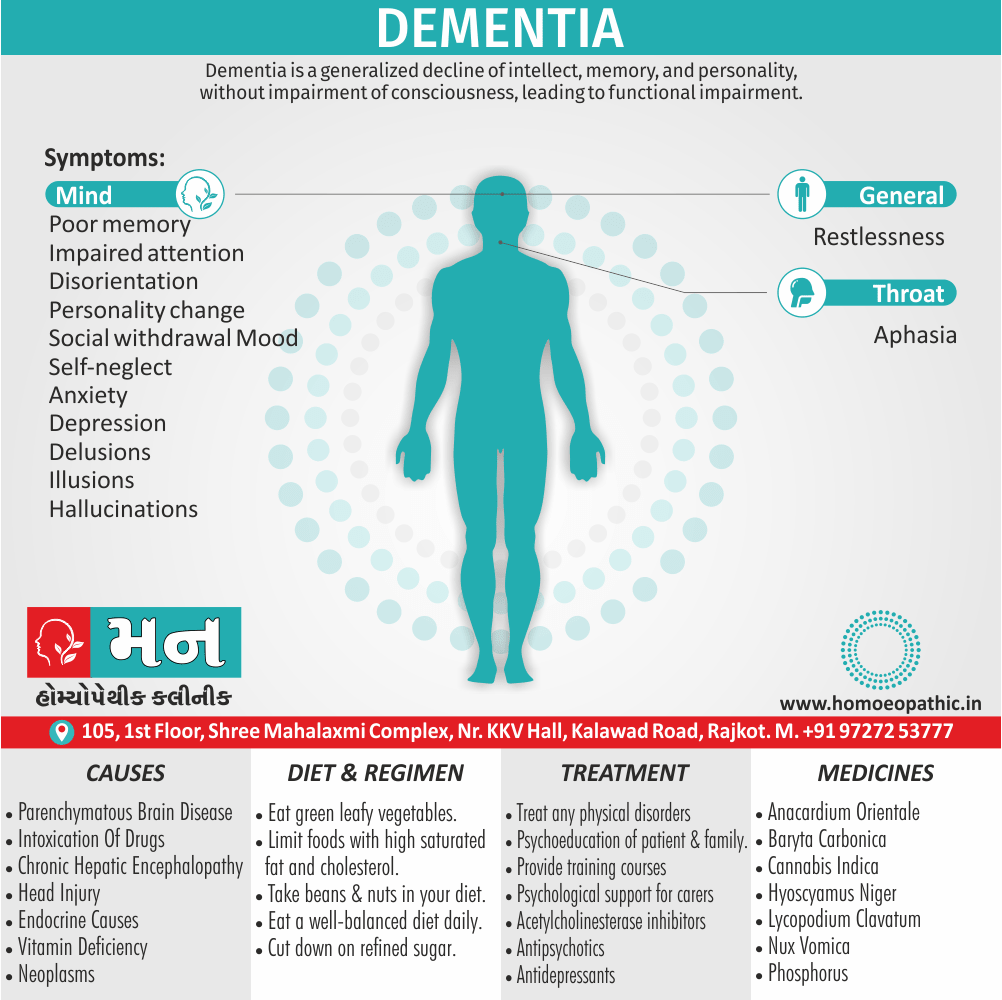
Dementia (F00-F03) is a syndrome due to disease of the brain, usually of a chronic or progressive nature, in which there is disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. Consciousness is not clouded. The impairments of cognitive function are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behaviour, or motivation. This syndrome occurs in Alzheimer disease, in cerebrovascular disease, and in other conditions primarily or secondarily affecting the brain.
- Use additional code, if desired, to identify the underlying disease.
F00*Dementia in Alzheimer disease (G30.-†)
- Alzheimer disease is a primary degenerative cerebral disease of unknown etiology with characteristic neuropathological and neurochemical features. The disorder is usually insidious in onset and develops slowly but steadily over a period of several years.
F00.0*Dementia in Alzheimer disease with early onset i.e. (G30.0†)
- Dementia in Alzheimer disease with onset before the age of 65, with a relatively rapid deteriorating course and with marked multiple disorders of the higher cortical functions.
- Alzheimer disease, type 2
- Presenile dementia, Alzheimer type
- Primary degenerative dementia of the Alzheimer type, presenile onset
F00.1*Dementia in Alzheimer disease with late onset i.e. (G30.1†)
- Dementia in Alzheimer disease with onset after the age of 65, usually in the late 70s or thereafter, with a slow progression, and with memory impairment as the principal feature.
- Alzheimer disease, type 1
- Primary degenerative dementia of the Alzheimer type, senile onset
- Senile dementia, Alzheimer type
F00.2*Dementia in Alzheimer disease, atypical or mixed type i.e. (G30.8†)
- Atypical dementia, Alzheimer type
F01Vascular dementia
- Vascular dementia is the result of infarction of the brain due to vascular disease, including hypertensive cerebrovascular disease. The infarcts are usually small but cumulative in their effect. Onset is usually in later life.
- Incl.:
- arteriosclerotic dementia
F01.0Vascular dementia of acute onset i.e.
- Usually develops rapidly after a succession of strokes from cerebrovascular thrombosis, embolism or haemorrhage. In rare cases, a single large infarction may be the cause.
F01.1Multi-infarct dementia i.e.
- Gradual in onset, following a number of transient ischaemic episodes which produce an accumulation of infarcts in the cerebral parenchyma.
- Predominantly cortical dementia
F01.2Subcortical vascular dementia i.e.
- Includes cases with a history of hypertension and foci of ischaemic destruction in the deep white matter of the cerebral hemispheres. The cerebral cortex is usually preserved and this contrasts with the clinical picture which may closely resemble that of dementia in Alzheimer disease.
F02*Dementia in other diseases classified elsewhere
- Cases of dementia due, or presumed to be due, to causes other than Alzheimer disease or cerebrovascular disease. Onset may be at any time in life, though rarely in old age.
F02.0*Dementia in Pick disease i.e. (G31.0†)
- A progressive dementia, commencing in middle age, characterized by early, slowly progressing changes of character and social deterioration, followed by impairment of intellect, memory, and language functions, with apathy, euphoria and, occasionally, extrapyramidal phenomena.
F02.1*Dementia in Creutzfeldt-Jakob disease i.e. (A81.0†)
- A progressive dementia with extensive neurological signs, due to specific neuropathological changes that are presumed to be caused by a transmissible agent. Onset is usually in middle or later life, but may be at any adult age. The course is subacute, leading to death within one to two years.
F02.2*Dementia in Huntington disease i.e. (G10†)
- A dementia occurring as part of a widespread degeneration of the brain. The disorder is transmitted by a single autosomal dominant gene. Symptoms typically emerge in the third and fourth decade. Progression is slow, leading to death usually within 10 to 15 years.
- Dementia in Huntington chorea
F02.3*Dementia in Parkinson disease i.e. (G20†)
- A dementia developing in the course of established Parkinson disease. No particular distinguishing clinical features have yet been demonstrated.
- Dementia in:
- paralysis agitans
- parkinsonism
F02.4*Dementia in human immunodeficiency virus [HIV] disease i.e. (B22.0†)
- Dementia developing in the course of HIV disease, in the absence of a concurrent illness or condition other than HIV infection that could explain the clinical features.
F02.8*Dementia in other specified diseases classified elsewhere i.e.
- Dementia (in) i.e.:
- cerebral lipidosis (E75.-†)
- epilepsy (G40.-†)
- hepatolenticular degeneration (E83.0†)
- hypercalcaemia (E83.5†)
- hypothyroidism, acquired (E01.-†, E03.-†)
- intoxications (T36-T65†)
- Lewy body (ies) (disease) (G31.8†)
- multiple sclerosis (G35†)
- neurosyphilis (A52.1†)
- niacin deficiency [pellagra] (E52†)
- polyarteritis nodosa (M30.0†)
- systemic lupus erythematosus (M32.-†)
- trypanosomiasis (B56.-†, B57.-†)
- uraemia (N18.5†)
- vitamin B12 deficiency (E53.8†)
F03Unspecified dementia
- Incl.:
- Presenile i.e.:
- dementia NOS
- psychosis NOS
- Primary degenerative dementia NOS
-
- dementia i.e.:
- NOS
- depressed or paranoid type
- psychosis NOS
- dementia i.e.:
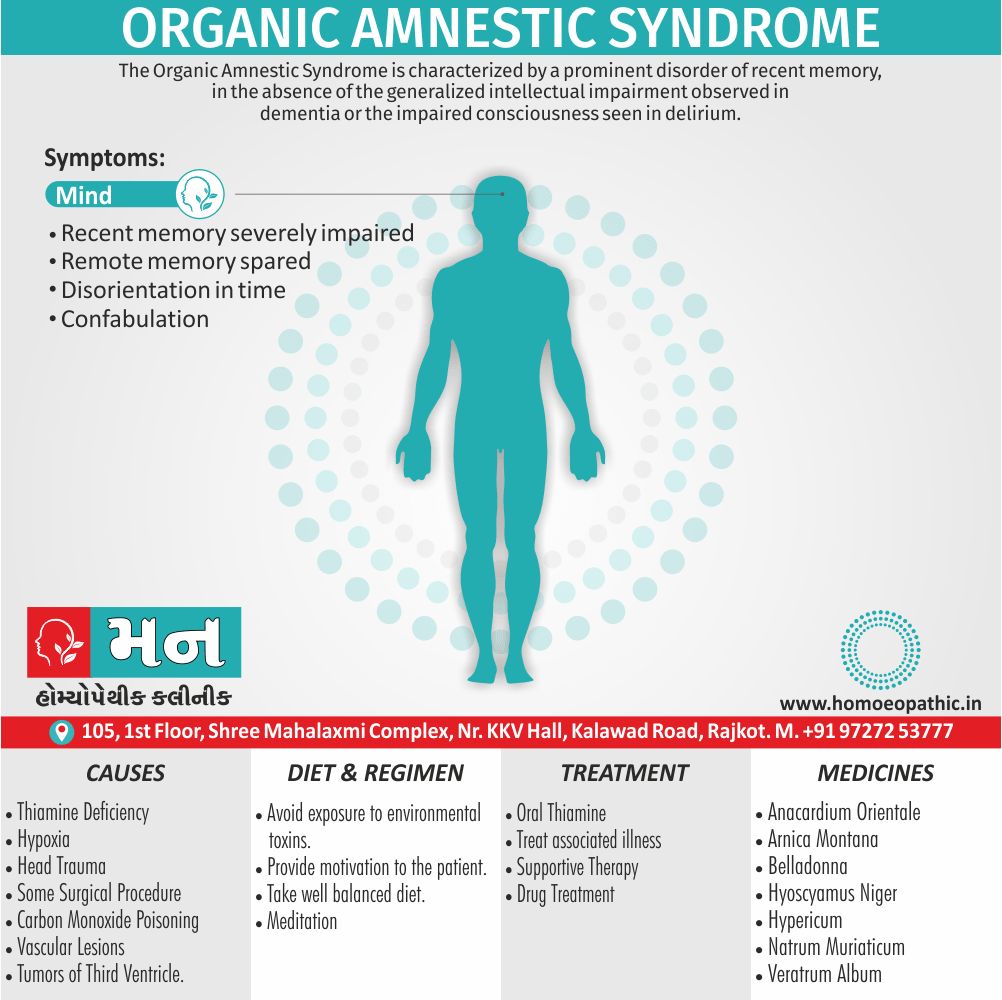
F04Organic amnesic syndrome, not induced by alcohol and other psychoactive substances
- A syndrome of prominent impairment of recent and remote memory while immediate recall is preserved, with reduced ability to learn new material and disorientation in time. Confabulation may be a marked feature, but perception and other cognitive functions, including the intellect, are usually intact. The prognosis depends on the course of the underlying lesion.
- Incl.:
- Korsakov psychosis or syndrome, nonalcoholic
- Excl.:
- amnesia i.e.:
- Korsakov syndrome i.e.:
- alcohol-induced or unspecified (F10.6)
- induced by other psychoactive substances (F11-F19 with common fourth character .6)
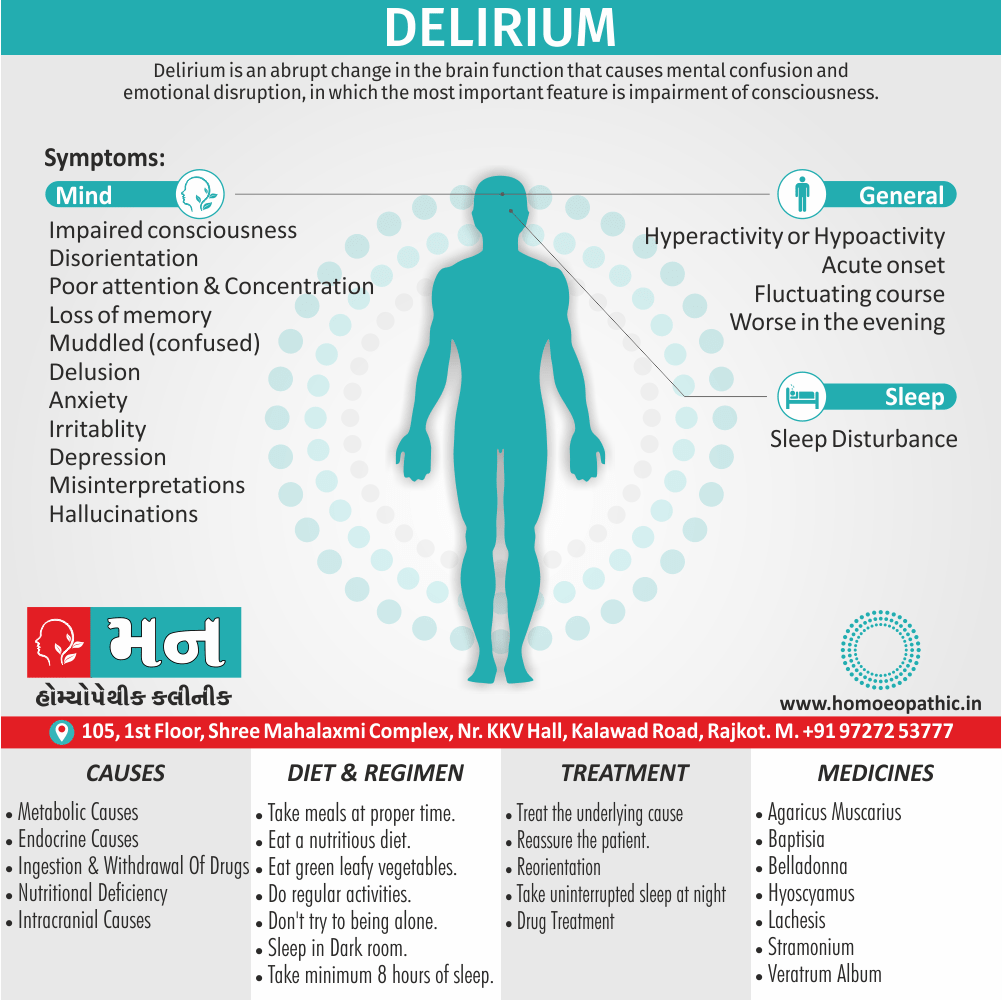
F05Delirium, not induced by alcohol and other psychoactive substances
- An etiologically nonspecific organic cerebral syndrome characterized by concurrent disturbances of consciousness and attention, perception, thinking, memory, psychomotor behaviour, emotion, and the sleep-wake schedule. The duration is variable and the degree of severity ranges from mild to very severe.
- Incl.:
- acute or subacute i.e.:
- brain syndrome
- confusional state (nonalcoholic)
- infective psychosis
- organic reaction
- psycho-organic syndrome
- Excl.:
- delirium tremens, alcohol-induced or unspecified (F10.4)
F05.0Delirium not superimposed on dementia, so described
F05.1Delirium superimposed on dementia
- Conditions meeting the above criteria but developing in the course of a dementia (F00-F03).
F05.8Other delirium
- Delirium of mixed origin
- Postoperative delirium
F05.9Delirium, unspecified
F06Other mental disorders due to brain damage and dysfunction and to physical disease
- Includes miscellaneous conditions causally related to brain disorder due to primary cerebral disease, to systemic disease affecting the brain secondarily, to exogenous toxic substances or hormones, to endocrine disorders, or to other somatic illnesses.
F06.0Organic hallucinosis
- A disorder of persistent or recurrent hallucinations, usually visual or auditory, that occur in clear consciousness and may or may not be recognized by the subject as such. Delusional elaboration of the hallucinations may occur, but delusions do not dominate the clinical picture; insight may be preserved.
- Organic hallucinatory state (nonalcoholic)
- Excl.:
- alcoholic hallucinosis (F10.5)
- schizophrenia (F20.-)
F06.1Organic catatonic disorder
- A disorder of diminished (stupor) or increased (excitement) psychomotor activity associated with catatonic symptoms. The extremes of psychomotor disturbance may alternate.
F06.2Organic delusional [schizophrenia-like] disorder
- A disorder in which persistent or recurrent delusions dominate the clinical picture. The delusions may be accompanied by hallucinations. Some features suggestive of schizophrenia, such as bizarre hallucinations or thought disorder, may be present.
- Paranoid also paranoid-hallucinatory organic states
- Schizophrenia-like psychosis in epilepsy
- Excl.:
- disorde i.e.:
- acute and transient psychotic (F23.-)
- persistent delusional (F22.-)
- psychotic drug-induced (F11-F19 with common fourth character .5)
- schizophrenia (F20.-)
F06.3Organic mood [affective] disorders
- Disorders characterized by a change in mood or affect, usually accompanied by a change in the overall level of activity, depressive, hypomanic, manic or bipolar (see F30-F38), but arising as a consequence of an organic disorder.
- Excl.:
- mood disorders, nonorganic or unspecified (F30-F39)
F06.4Organic anxiety disorder
- A disorder characterized by the essential descriptive features of a generalized anxiety disorder (F41.1), a panic disorder (F41.0), or a combination of both, but arising as a consequence of an organic disorder.
- Excl.:
- anxiety disorders, nonorganic or unspecified (F41.-)
F06.5Organic dissociative disorder
- A disorder characterized by a partial or complete loss of the normal integration between memories of the past, awareness of identity and immediate sensations, and control of bodily movements (see F44.-), but arising as a consequence of an organic disorder.
- Excl.:
- dissociative [conversion] disorders, nonorganic or unspecified (F44.-)
F06.6Organic emotionally labile [asthenic] disorder
- A disorder characterized by emotional incontinence or lability, fatigability, and a variety of unpleasant physical sensations (e.g. dizziness) and pains, but arising as a consequence of an organic disorder.
- Excl.:
- somatoform disorders, nonorganic or unspecified (F45.-)
F06.7Mild cognitive disorder
- A disorder characterized by impairment of memory, learning difficulties, and reduced ability to concentrate on a task for more than brief periods. There is often a marked feeling of mental fatigue when mental tasks are attempted, and new learning is found to be subjectively difficult even when objectively successful. None of these symptoms is so severe that a diagnosis of either dementia (F00-F03) or delirium (F05.-) can be made. This diagnosis should be made only in association with a specified physical disorder, and should not be made in the presence of any of the mental or behavioural disorders classified to F10-F99. The disorder may precede, accompany, or follow a wide variety of infections and physical disorders, both cerebral and systemic, but direct evidence of cerebral involvement is not necessarily present. It can be differentiated from postencephalitic syndrome (F07.1) and postconcussional syndrome (F07.2) by its different etiology, more restricted range of generally milder symptoms, and usually shorter duration.
F06.8Other specified mental disorders due to brain damage and dysfunction and to physical disease
- Epileptic psychosis NOS
F06.9Unspecified mental disorder due to brain damage and dysfunction and to physical disease
- Organic:
- brain syndrome NOS
- mental disorder NOS
F07Personality and behavioural disorders due to brain disease, damage and dysfunction
- Alteration of personality and behaviour can be a residual or concomitant disorder of brain disease, damage or dysfunction.
F07.0Organic personality disorder
- A disorder characterized by a significant alteration of the habitual patterns of behaviour displayed by the subject premorbidly, involving the expression of emotions, needs also impulses. Impairment of cognitive and thought functions, also altered sexuality may also be part of the clinical picture.
- Organic e.g.:
- pseudopsychopathic personality
- pseudoretarded personality
- Syndrome e.g.:
- frontal lobe
- limbic epilepsy personality
- lobotomy
- postleucotomy
F07.1Postencephalitic syndrome
- Residual nonspecific also variable behavioural change following recovery from either viral or bacterial encephalitis. Besides this; The principal difference between this disorder and the organic personality disorders is that it is reversible.
- Excl.:
- organic personality disorder (F07.0)
F07.2Postconcussional syndrome
- A syndrome that occurs following head trauma (usually sufficiently severe to result in loss of consciousness) and includes a number of disparate symptoms such as headache, dizziness, fatigue, irritability, difficulty in concentration and performing mental tasks, impairment of memory, insomnia, and reduced tolerance to stress, emotional excitement, or alcohol.
- Postcontusional syndrome (in other words; encephalopathy)
- Post-traumatic brain syndrome, nonpsychotic
- Excl.:
- current concussion, brain (S06.0)
F07.8Other organic personality and behavioural disorders due to brain disease, damage and dysfunction
- Right hemispheric organic affective disorder
F07.9Unspecified organic personality and behavioural disorder due to brain disease, damage and dysfunction
- Organic psychosyndrome
F09Unspecified organic or symptomatic mental disorder
- Incl.:
- Psychosis:
- organic NOS
- symptomatic NOS
- Excl.:
- psychosis NOS (F29)
Frequently Asked Questions
What is Organic Mental Disorders?
It is assumed that all psychological and behavioural processes, whether normal or abnormal, are a result of normal or deranged brain function.
What are the types of Organic Mental Disorders?
- Those due to a known organic cause.
- Those in whose causation an organic factor has not yet been found or proven.
- Those primarily due to unpredictable social factors.
Definition:
In Organic Mental Disorders, it is assumed that all psychological and behavioural processes, whether normal or abnormal, are a result of normal or deranged brain function. A rational corollary would be that all psychiatric disorders are due to abnormal brain functioning and are therefore organic. However, this would be a gross oversimplification.
Overview
Epidemiology
Causes
Risk Factors
Pathogenesis
Pathophysiology
Types
Clinical Features
Sign & Symptoms
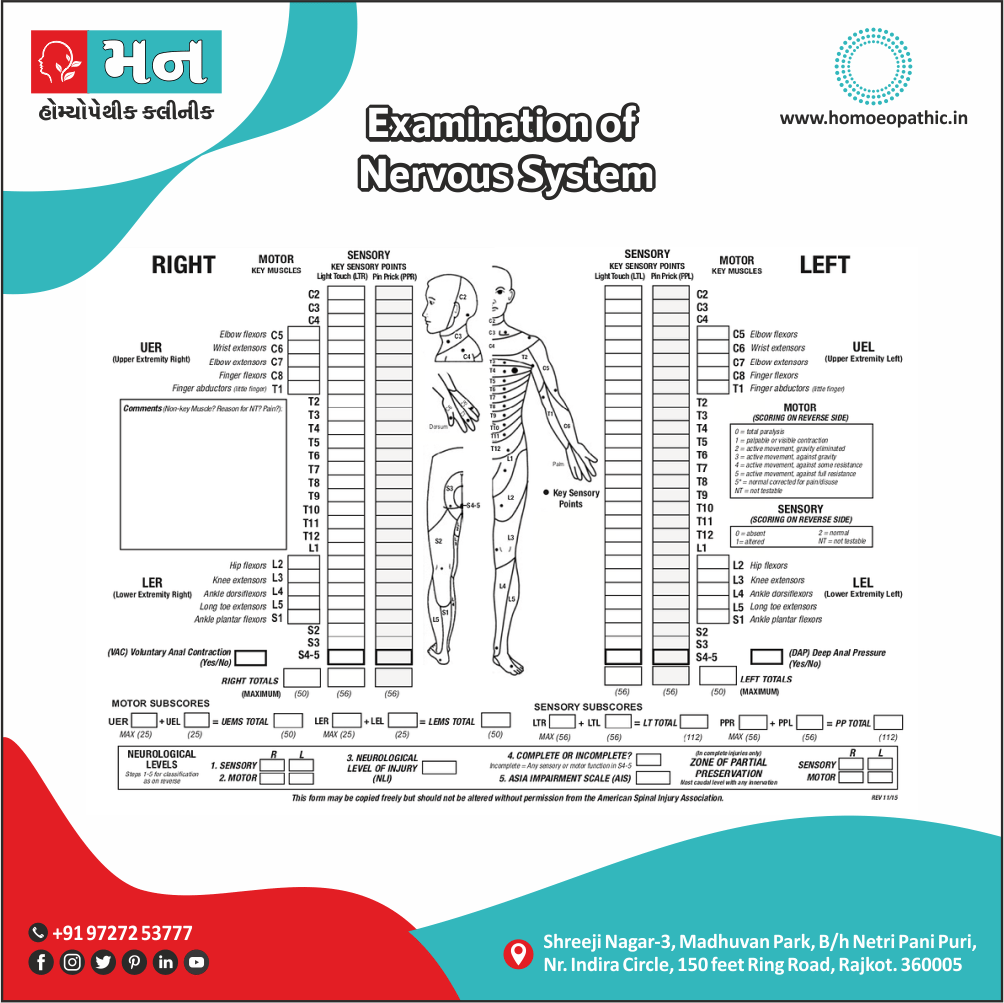
Clinical Examination
Diagnosis
Differential Diagnosis
Complications
Investigations
Treatment
Prevention
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Terminology
References
FAQ
Also Search As
Classification
Overview
AAA
Epidemiology
Indian epidemiology then other
Causes
This refers to the initiating factors that trigger a disease process.
- Examples of causes include:
- Pathogens: Viruses, bacteria, fungi, parasites (infectious diseases)
- Genetic mutations: Inherited or spontaneous changes in genes (genetic diseases)
- Environmental factors: Toxins, radiation, nutritional deficiencies
- Lifestyle choices: Smoking, unhealthy diet, lack of exercise (contributing factors)
Risk Factors
Risk factors are things that make you more likely to develop a disease in the first place.
Pathogenesis
Pathogenesis refers to the development of a disease. It’s the story of how a disease gets started and progresses.
This is the entire journey of a disease, encompassing the cause but going beyond it.
Pathophysiology
Pathophysiology, on the other hand, focuses on the functional changes that occur in the body due to the disease. It explains how the disease disrupts normal physiological processes and how this disruption leads to the signs and symptoms we see.
Imagine a car accident. Pathogenesis would be like understanding how the accident happened – what caused it, the sequence of events (e.g., one car ran a red light, then hit another car). Pathophysiology would be like understanding the damage caused by the accident – the bent fenders, deployed airbags, and any injuries to the passengers.
In simpler terms, pathogenesis is about the "why" of a disease, while pathophysiology is about the "how" of the disease’s effects.
Types
Types of Organic Mental Disorders:
According to our present knowledge, there are broadly three types of psychiatric disorders:
- Those due to a known organic cause.
- Those in whose causation an organic factor has not yet been found or proven.
- Those primarily due to unpredictable social factors.
Only disorders with a known organic cause are called organic mental disorders. Thus, organic mental
disorders are behavioural or psychological disorders associated with transient or permanent brain dysfunction and include only those mental and behavioural disorders that are due to demonstrable cerebral disease or disorder, either primary (primary brain pathology) or secondary (brain dysfunction due to systemic diseases). The use of term organic here does not imply that other psychiatric disorders are ‘non-organic’ in the sense of having no biological basis. It simply means that the organic mental disorders have a demonstrable and independently diagnosable cerebral disease or disorder, unlike other psychiatric disorders that do not at present.
Since organic brain illness can mimic any psychiatric disorder, especially in the initial stages, organic mental disorder should be the first consideration in evaluating a patient with any psychological or behavioural clinical syndrome. The presence of following features requires a high index of suspicion for an organic mental disorder (or what is loosely called as organicity):
- First episode.
- Sudden onset.
- Older age of onset.
- History of drug and/or alcohol use disorder.
- Concurrent medical or neurological illness.
- Neurological symptoms or signs, such as seizures, impairment of consciousness, head injury, sensory or motor disturbance.
- Presence of confusion, disorientation, memory impairment or soft neurological signs.
- Prominent visual or other non-auditory (e.g. olfactory, gustatory or tactile) hallucinations.
These disorders can be broadly sub-categorised into the following categories:
Clinical Features
Tab Content
Sign & Symptoms
Tab Content
Clinical Examination
Tab Content
Diagnosis
Tab Content
Differential Diagnosis
Complications
Complications are what happen after you have a disease. They are the negative consequences of the disease process.
Investigations
Tab Content
Treatment
Tab Content
Prevention
Tab Content
Homeopathic Treatment
Diet & Regimen
Do’s and Dont’s
Tab Content
Terminology
Tab Content
References
FAQ
Also Search As
Classification
Other Classification of Organic Mental Disorders:
International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10)-WHO Version for ;2016
Chapter V
Mental and behavioural disorders
(F00-F99)
Organic, including symptomatic, mental disorders
(F00-F09)
- This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable etiology in cerebral disease, brain injury, or other insult leading to cerebral dysfunction. Additionally; The dysfunction may be primary, as in diseases, injuries, and insults that affect the brain directly also selectively; or secondary, as in systemic diseases and disorders that attack the brain only as one of the multiple organs or systems of the body that are involved.
Dementia (F00-F03) is a syndrome due to disease of the brain, usually of a chronic or progressive nature, in which there is disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. Consciousness is not clouded. The impairments of cognitive function are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behaviour, or motivation. This syndrome occurs in Alzheimer disease, in cerebrovascular disease, and in other conditions primarily or secondarily affecting the brain.
- Use additional code, if desired, to identify the underlying disease.
F00*Dementia in Alzheimer disease (G30.-†)
- Alzheimer disease is a primary degenerative cerebral disease of unknown etiology with characteristic neuropathological and neurochemical features. The disorder is usually insidious in onset and develops slowly but steadily over a period of several years.
F00.0*Dementia in Alzheimer disease with early onset i.e. (G30.0†)
- Dementia in Alzheimer disease with onset before the age of 65, with a relatively rapid deteriorating course and with marked multiple disorders of the higher cortical functions.
- Alzheimer disease, type 2
- Presenile dementia, Alzheimer type
- Primary degenerative dementia of the Alzheimer type, presenile onset
F00.1*Dementia in Alzheimer disease with late onset i.e. (G30.1†)
- Dementia in Alzheimer disease with onset after the age of 65, usually in the late 70s or thereafter, with a slow progression, and with memory impairment as the principal feature.
- Alzheimer disease, type 1
- Primary degenerative dementia of the Alzheimer type, senile onset
- Senile dementia, Alzheimer type
F00.2*Dementia in Alzheimer disease, atypical or mixed type i.e. (G30.8†)
- Atypical dementia, Alzheimer type
F01Vascular dementia
- Vascular dementia is the result of infarction of the brain due to vascular disease, including hypertensive cerebrovascular disease. The infarcts are usually small but cumulative in their effect. Onset is usually in later life.
- Incl.:
- arteriosclerotic dementia
F01.0Vascular dementia of acute onset i.e.
- Usually develops rapidly after a succession of strokes from cerebrovascular thrombosis, embolism or haemorrhage. In rare cases, a single large infarction may be the cause.
F01.1Multi-infarct dementia i.e.
- Gradual in onset, following a number of transient ischaemic episodes which produce an accumulation of infarcts in the cerebral parenchyma.
- Predominantly cortical dementia
F01.2Subcortical vascular dementia i.e.
- Includes cases with a history of hypertension and foci of ischaemic destruction in the deep white matter of the cerebral hemispheres. The cerebral cortex is usually preserved and this contrasts with the clinical picture which may closely resemble that of dementia in Alzheimer disease.
F02*Dementia in other diseases classified elsewhere
- Cases of dementia due, or presumed to be due, to causes other than Alzheimer disease or cerebrovascular disease. Onset may be at any time in life, though rarely in old age.
F02.0*Dementia in Pick disease i.e. (G31.0†)
- A progressive dementia, commencing in middle age, characterized by early, slowly progressing changes of character and social deterioration, followed by impairment of intellect, memory, and language functions, with apathy, euphoria and, occasionally, extrapyramidal phenomena.
F02.1*Dementia in Creutzfeldt-Jakob disease i.e. (A81.0†)
- A progressive dementia with extensive neurological signs, due to specific neuropathological changes that are presumed to be caused by a transmissible agent. Onset is usually in middle or later life, but may be at any adult age. The course is subacute, leading to death within one to two years.
F02.2*Dementia in Huntington disease i.e. (G10†)
- A dementia occurring as part of a widespread degeneration of the brain. The disorder is transmitted by a single autosomal dominant gene. Symptoms typically emerge in the third and fourth decade. Progression is slow, leading to death usually within 10 to 15 years.
- Dementia in Huntington chorea
F02.3*Dementia in Parkinson disease i.e. (G20†)
- A dementia developing in the course of established Parkinson disease. No particular distinguishing clinical features have yet been demonstrated.
Dementia in:
- paralysis agitans
- parkinsonism
F02.4*Dementia in human immunodeficiency virus [HIV] disease i.e. (B22.0†)
- Dementia developing in the course of HIV disease, in the absence of a concurrent illness or condition other than HIV infection that could explain the clinical features.
F02.8*Dementia in other specified diseases classified elsewhere i.e.
Dementia (in) i.e.:
- cerebral lipidosis (E75.-†)
- epilepsy (G40.-†)
- hepatolenticular degeneration (E83.0†)
- hypercalcaemia (E83.5†)
- hypothyroidism, acquired (E01.-†, E03.-†)
- intoxications (T36-T65†)
- Lewy body (ies) (disease) (G31.8†)
- multiple sclerosis (G35†)
- neurosyphilis (A52.1†)
- niacin deficiency [pellagra] (E52†)
- polyarteritis nodosa (M30.0†)
- systemic lupus erythematosus (M32.-†)
- trypanosomiasis (B56.-†, B57.-†)
- uraemia (N18.5†)
- vitamin B12 deficiency (E53.8†)
F03Unspecified dementia
- Incl.:
Presenile i.e.:
- dementia NOS
- psychosis NOS
- Primary degenerative dementia NOS
- dementia i.e.:
- NOS
- depressed or paranoid type
- psychosis NOS
- dementia i.e.:
F04Organic amnesic syndrome, not induced by alcohol and other psychoactive substances
- A syndrome of prominent impairment of recent and remote memory while immediate recall is preserved, with reduced ability to learn new material and disorientation in time. Confabulation may be a marked feature, but perception and other cognitive functions, including the intellect, are usually intact. The prognosis depends on the course of the underlying lesion.
- Incl.:
- Korsakov psychosis or syndrome, nonalcoholic
- Excl.:
amnesia i.e.:
Korsakov syndrome i.e.:
- alcohol-induced or unspecified (F10.6)
- induced by other psychoactive substances (F11-F19 with common fourth character .6)
F05Delirium, not induced by alcohol and other psychoactive substances
- An etiologically nonspecific organic cerebral syndrome characterized by concurrent disturbances of consciousness and attention, perception, thinking, memory, psychomotor behaviour, emotion, and the sleep-wake schedule. The duration is variable and the degree of severity ranges from mild to very severe.
- Incl.:
acute or subacute i.e.:
- brain syndrome
- confusional state (nonalcoholic)
- infective psychosis
- organic reaction
- psycho-organic syndrome
- Excl.:
- delirium tremens, alcohol-induced or unspecified (F10.4)
F05.0Delirium not superimposed on dementia, so described
F05.1Delirium superimposed on dementia
- Conditions meeting the above criteria but developing in the course of a dementia (F00-F03).
F05.8Other delirium
- Delirium of mixed origin
- Postoperative delirium
F05.9Delirium, unspecified
F06Other mental disorders due to brain damage and dysfunction and to physical disease
- Includes miscellaneous conditions causally related to brain disorder due to primary cerebral disease, to systemic disease affecting the brain secondarily, to exogenous toxic substances or hormones, to endocrine disorders, or to other somatic illnesses.
F06.0Organic hallucinosis
- A disorder of persistent or recurrent hallucinations, usually visual or auditory, that occur in clear consciousness and may or may not be recognized by the subject as such. Delusional elaboration of the hallucinations may occur, but delusions do not dominate the clinical picture; insight may be preserved.
- Organic hallucinatory state (nonalcoholic)
- Excl.:
- alcoholic hallucinosis (F10.5)
- schizophrenia (F20.-)
F06.1Organic catatonic disorder
- A disorder of diminished (stupor) or increased (excitement) psychomotor activity associated with catatonic symptoms. The extremes of psychomotor disturbance may alternate.
F06.2Organic delusional [schizophrenia-like] disorder
- A disorder in which persistent or recurrent delusions dominate the clinical picture. The delusions may be accompanied by hallucinations. Some features suggestive of schizophrenia, such as bizarre hallucinations or thought disorder, may be present.
- Paranoid also paranoid-hallucinatory organic states
- Schizophrenia-like psychosis in epilepsy
- Excl.:
disorde i.e.:
- acute and transient psychotic (F23.-)
- persistent delusional (F22.-)
- psychotic drug-induced (F11-F19 with common fourth character .5)
- schizophrenia (F20.-)
F06.3Organic mood [affective] disorders
- Disorders characterized by a change in mood or affect, usually accompanied by a change in the overall level of activity, depressive, hypomanic, manic or bipolar (see F30-F38), but arising as a consequence of an organic disorder.
- Excl.:
- mood disorders, nonorganic or unspecified (F30-F39)
F06.4Organic anxiety disorder
- A disorder characterized by the essential descriptive features of a generalized anxiety disorder (F41.1), a panic disorder (F41.0), or a combination of both, but arising as a consequence of an organic disorder.
- Excl.:
- anxiety disorders, nonorganic or unspecified (F41.-)
F06.5Organic dissociative disorder
- A disorder characterized by a partial or complete loss of the normal integration between memories of the past, awareness of identity and immediate sensations, and control of bodily movements (see F44.-), but arising as a consequence of an organic disorder.
- Excl.:
- dissociative [conversion] disorders, nonorganic or unspecified (F44.-)
F06.6Organic emotionally labile [asthenic] disorder
- A disorder characterized by emotional incontinence or lability, fatigability, and a variety of unpleasant physical sensations (e.g. dizziness) and pains, but arising as a consequence of an organic disorder.
- Excl.:
- somatoform disorders, nonorganic or unspecified (F45.-)
F06.7Mild cognitive disorder
- A disorder characterized by impairment of memory, learning difficulties, and reduced ability to concentrate on a task for more than brief periods. There is often a marked feeling of mental fatigue when mental tasks are attempted, and new learning is found to be subjectively difficult even when objectively successful. None of these symptoms is so severe that a diagnosis of either dementia (F00-F03) or delirium (F05.-) can be made. This diagnosis should be made only in association with a specified physical disorder, and should not be made in the presence of any of the mental or behavioural disorders classified to F10-F99. The disorder may precede, accompany, or follow a wide variety of infections and physical disorders, both cerebral and systemic, but direct evidence of cerebral involvement is not necessarily present. It can be differentiated from postencephalitic syndrome (F07.1) and postconcussional syndrome (F07.2) by its different etiology, more restricted range of generally milder symptoms, and usually shorter duration.
F06.8Other specified mental disorders due to brain damage and dysfunction and to physical disease
- Epileptic psychosis NOS
F06.9Unspecified mental disorder due to brain damage and dysfunction and to physical disease
Organic:
- brain syndrome NOS
- mental disorder NOS
F07Personality and behavioural disorders due to brain disease, damage and dysfunction
- Alteration of personality and behaviour can be a residual or concomitant disorder of brain disease, damage or dysfunction.
F07.0Organic personality disorder
- A disorder characterized by a significant alteration of the habitual patterns of behaviour displayed by the subject premorbidly, involving the expression of emotions, needs also impulses. Impairment of cognitive and thought functions, also altered sexuality may also be part of the clinical picture.
Organic e.g.:
- pseudopsychopathic personality
- pseudoretarded personality
Syndrome e.g.:
- frontal lobe
- limbic epilepsy personality
- lobotomy
- postleucotomy
F07.1Postencephalitic syndrome
- Residual nonspecific also variable behavioural change following recovery from either viral or bacterial encephalitis. Besides this; The principal difference between this disorder and the organic personality disorders is that it is reversible.
- Excl.:
- organic personality disorder (F07.0)
F07.2Postconcussional syndrome
- A syndrome that occurs following head trauma (usually sufficiently severe to result in loss of consciousness) and includes a number of disparate symptoms such as headache, dizziness, fatigue, irritability, difficulty in concentration and performing mental tasks, impairment of memory, insomnia, and reduced tolerance to stress, emotional excitement, or alcohol.
- Postcontusional syndrome (in other words; encephalopathy)
- Post-traumatic brain syndrome, nonpsychotic
- Excl.:
- current concussion, brain (S06.0)
F07.8Other organic personality and behavioural disorders due to brain disease, damage and dysfunction
- Right hemispheric organic affective disorder
F07.9Unspecified organic personality and behavioural disorder due to brain disease, damage and dysfunction
- Organic psychosyndrome
F09Unspecified organic or symptomatic mental disorder
- Incl.:
Psychosis:
- organic NOS
- symptomatic NOS
- Excl.:
- psychosis NOS (F29)
Frequently Asked Questions (FAQ)
XYZ
XXX
XYZ
XXX
XYZ
XXX
How can I find reputable homeopathy clinics or homeopathic doctors in my area?
You can found Homeopathic Clinic For XXXX by searching for
Specific city Examples are
You can also search for near you Examples are